Division of Surgical Oncology, Center for Patient Care and Outcomes Research, Medical College of Wisconsin, Milwaukee.
Division of Biostatistics, Center for Patient Care and Outcomes Research, Medical College of Wisconsin, Milwaukee.
JAMA Surg. 2014 Feb;149(2):185-92. doi: 10.1001/jamasurg.2013.4350.
Sentinel lymph node biopsy (SLNB) is the standard of care for axillary staging in patients with clinically node-negative breast cancer. It is not known whether SLNB rates differ by surgeon expertise. If surgeons with less breast cancer expertise are less likely to offer SLNB to these patients, this practice pattern could lead to unnecessary axillary lymph node dissections and lymphedema.
To explore potential measures of surgical expertise (including a novel objective specialization measure: percentage of a surgeon's operations performed for breast cancer determined from Medicare claims) on the use of SLNB for invasive breast cancer.
DESIGN, SETTING, AND POPULATION: A population-based prospective cohort study was conducted in California, Florida, and Illinois. Participants included elderly (65-89 years) women identified from Medicare claims as having had incident invasive breast cancer surgery in 2003. Patient, tumor, treatment, and surgeon characteristics were examined.
Type of axillary surgery performed.
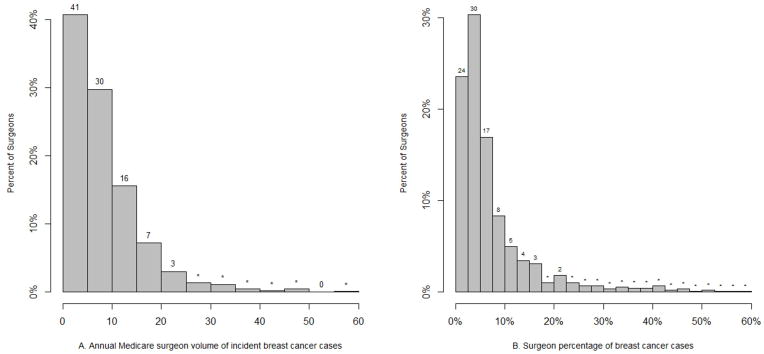
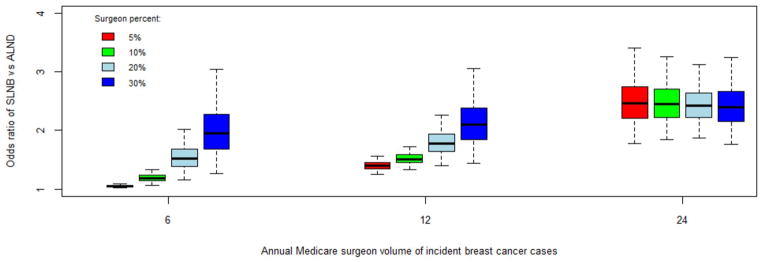
Of 1703 women who received treatment by 863 surgeons, 56.4% underwent an initial SLNB, 37.2% initial axillary lymph node dissection, and 6.3% no axillary surgery. The median annual surgeon Medicare volume of breast cancer cases was 6.0 (range, 1.5-57.0); the median surgeon percentage of breast cancer cases was 4.5% (range, 0.4%-100.0%). After multivariable adjustment of patient and surgeon factors, women operated on by surgeons with higher volumes and percentages of breast cancer cases had a higher likelihood of undergoing SLNB. Specifically, women were most likely to undergo SLNB if the operation was performed by high-volume surgeons (regardless of percentage) or by lower-volume surgeons with a high percentage of breast cancer cases. In addition, membership in the American Society of Breast Surgeons (odds ratio, 1.98; 95% CI, 1.51-2.60) and Society of Surgical Oncology (1.59; 1.09-2.30) were independent predictors of women undergoing an initial SLNB.
Patients who receive treatment from surgeons with more experience with and focus on breast cancer are significantly more likely to undergo SLNB, highlighting the importance of receiving initial treatment by specialized providers. Factors relating to specialization in a particular area, including our novel surgeon percentage measure, require further investigation as potential indicators of quality of care.
前哨淋巴结活检(SLNB)是临床阴性乳腺癌腋窝分期的标准治疗方法。目前尚不清楚外科医生的专业水平是否会影响 SLNB 的使用率。如果专业水平较低的外科医生不太可能向这些患者提供 SLNB,那么这种治疗模式可能会导致不必要的腋窝淋巴结清扫和淋巴水肿。
探讨外科医生专业水平(包括一种新的客观专业衡量标准:从医疗保险索赔中确定外科医生进行的乳腺癌手术百分比)对浸润性乳腺癌 SLNB 使用的影响。
设计、地点和人群:这是一项在加利福尼亚州、佛罗里达州和伊利诺伊州进行的基于人群的前瞻性队列研究。参与者包括从医疗保险索赔中确定的 65-89 岁患有浸润性乳腺癌手术的老年女性。研究人员分析了患者、肿瘤、治疗和外科医生的特征。
实施的腋窝手术类型。
在接受 863 名外科医生治疗的 1703 名女性中,56.4%的女性接受了初始 SLNB,37.2%的女性接受了初始腋窝淋巴结清扫术,6.3%的女性未进行腋窝手术。外科医生每年接受乳腺癌治疗的中位数为 6.0(范围为 1.5-57.0);外科医生乳腺癌病例的中位数百分比为 4.5%(范围为 0.4%-100.0%)。在对患者和外科医生因素进行多变量调整后,由手术量和乳腺癌病例百分比较高的外科医生进行手术的女性更有可能接受 SLNB。具体而言,如果手术是由高手术量的外科医生(无论百分比如何)或手术量较低但乳腺癌病例百分比较高的外科医生进行的,那么女性最有可能接受 SLNB。此外,美国乳腺外科学会(ASBrS)(比值比,1.98;95%置信区间,1.51-2.60)和外科肿瘤学会(SOS)(1.59;1.09-2.30)的成员资格是女性接受初始 SLNB 的独立预测因素。
接受经验丰富且专注于乳腺癌治疗的外科医生治疗的患者,更有可能接受 SLNB,这突出了接受专业治疗提供者初始治疗的重要性。与特定领域专业化相关的因素,包括我们新的外科医生百分比衡量标准,需要进一步调查,作为护理质量的潜在指标。