De Crea C, Raffaelli M, Traini E, Giustozzi E, Oragano L, Bellantone R, Lombardi C P
UO di Chirurgia Endocrina e Metabolica, Università Cattolica del S. Cuore, Policlinico A. Gemelli, Rome, Italy.
Acta Otorhinolaryngol Ital. 2013 Dec;33(6):388-92.
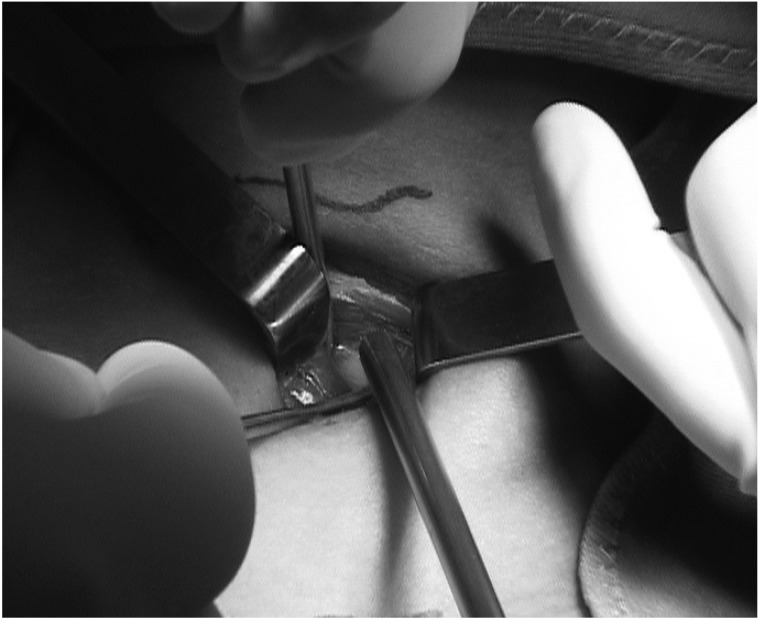
Minimally-invasive procedures for parathyroidectomy have revolutionized the surgical treatment of primary hyperparathyroidism (pHPT). Coexistence of goitre is considered a major contraindication for these approaches, especially if unilateral. A specific advantage of video-assisted parathyroidectomy (VAP) compared to other endoscopic techniques is the possibility to combine it with thyroidectomy when necessary and when the selection criteria for video-assisted thyroidectomy (VAT) are met. We evaluated the role of VAP in a region with a high prevalence of goitre. The medical records of all patients who underwent parathyroidectomy and concomitant thyroid resection in our Division, between May 1998 and June 2012, were reviewed. Patients who underwent VAP and concomitant VAT were included in this study. Overall, in this period, 615 patients were treated in our Division for pHPT and 227 patients (36.9%) underwent concomitant thyroid resection. Among these, 384 patients were selected for VAP and 124 (32.3%) underwent concomitant VAT (lobectomy in 26 cases, total thyroidectomy in 98). No conversion to conventional surgery was registered. Mean operative time was 66.6 ± 43.6 min. Transient hypocalcaemia was observed in 42 cases. A transient recurrent nerve lesion was registered in one case. No other complications occurred. Final histology showed parathyroid adenoma in all but two cases of parathyroid carcinoma, benign goitre in 119 cases and papillary thyroid carcinoma in the remaining 5 patients. After a mean follow-up of 33.2 months, no persistent or recurrent disease was observed. In our experience, a video-assisted approach for the treatment of synchronous thyroid and parathyroid diseases is feasible, effective and safe at least considering short-term follow-up.
甲状旁腺切除术的微创手术彻底改变了原发性甲状旁腺功能亢进症(pHPT)的外科治疗方法。甲状腺肿的并存被认为是这些手术方法的主要禁忌症,尤其是单侧甲状腺肿。与其他内镜技术相比,视频辅助甲状旁腺切除术(VAP)的一个特殊优势是,在必要且符合视频辅助甲状腺切除术(VAT)的选择标准时,可以将其与甲状腺切除术相结合。我们评估了VAP在甲状腺肿高发地区的作用。回顾了1998年5月至2012年6月期间在我们科室接受甲状旁腺切除术及同期甲状腺切除术的所有患者的病历。本研究纳入了接受VAP及同期VAT的患者。在此期间,我们科室共治疗了615例pHPT患者,其中227例(36.9%)接受了同期甲状腺切除术。其中,384例患者选择了VAP,124例(32.3%)接受了同期VAT(26例行叶切除术,98例行全甲状腺切除术)。未记录到转为传统手术的情况。平均手术时间为66.6±43.6分钟。42例患者出现短暂性低钙血症。1例患者记录有短暂性喉返神经损伤。未发生其他并发症。最终组织学检查显示,除2例甲状旁腺癌外,其余均为甲状旁腺腺瘤,119例为良性甲状腺肿,其余5例为甲状腺乳头状癌。平均随访33.2个月后,未观察到持续性或复发性疾病。根据我们的经验,至少从短期随访来看,视频辅助方法治疗同步性甲状腺和甲状旁腺疾病是可行、有效且安全的。