Hawaii Center for AIDS, University of Hawaii, Honolulu, HI, USA; Department of Tropical Medicine, John A. Burns School of Medicine, Honolulu, HI, USA.
Hawaii Center for AIDS, University of Hawaii, Honolulu, HI, USA; Department of Tropical Medicine, John A. Burns School of Medicine, Honolulu, HI, USA.
Atherosclerosis. 2014 Jan;232(1):52-8. doi: 10.1016/j.atherosclerosis.2013.10.021. Epub 2013 Oct 31.
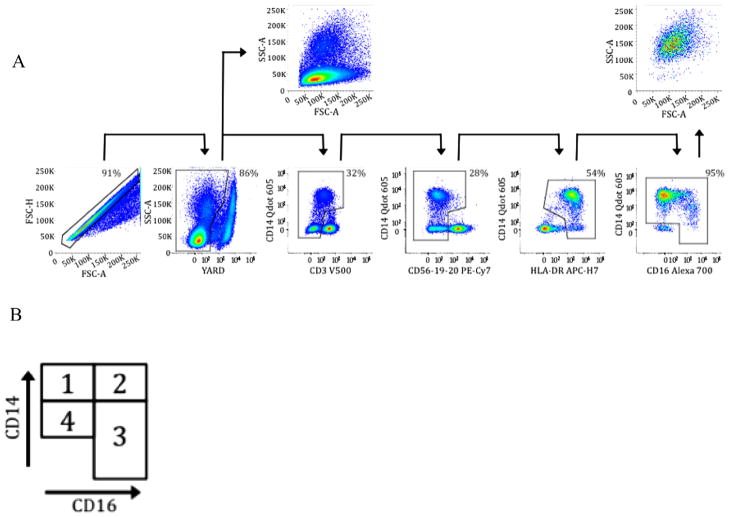
HIV infection causes systemic immune inflammation, and increases the risk for cardiovascular (CVD) disease even among those on virologically suppressive anti-retroviral treatment (ART). We performed a biostatistical analysis and screen of candidate cellular and plasma biomarkers for association with carotid artery intima-media thickness (CIMT), independent of traditional CVD risk factors such as age, gender, systolic blood pressure (SBP), lipid levels, smoking and diabetes. We conducted a multi-stage analysis based on a cross-sectional study of CVD risk in HIV-infected subjects age >45 years on ART for >6 months. The goal of this analysis was to identify candidate cellular and plasma biomarkers of CIMT in HIV-1 infected adults. We further sought to determine if these candidate biomarkers were independent of traditional CVD risk factors previously identified in HIV negative adults. High-resolution B-mode ultrasound images of the right common carotid common artery (CCA) were obtained. Plasma soluble inflammatory mediators, cytokines and chemokines were detected. Monocytes were defined by CD14/CD16 expression, and CD8+ T-cell activation by CD38/HLA-DR expression. Subjects were a median of 49.5 years old, 87% male, had a CIMT of 0.73 mm, FRS of 6%, a median viral load of 48 copies/mL, and CD4+ T cell count of 479 cells/μL. Soluble VCAM-1, and expansion of CD14dimCD16- monocytes each associated with higher CIMT independently of age and SBP. These factors are distinct components of a shared atherogenic process; 1) vascular endothelial molecular expression and 2) vascular monocytes that enter into the vascular endothelium and promote atherosclerotic plaque.
HIV 感染会引起全身免疫炎症,即使在接受病毒学抑制性抗逆转录病毒治疗(ART)的患者中,也会增加心血管疾病(CVD)的风险。我们进行了生物统计学分析和候选细胞及血浆生物标志物的筛选,这些标志物与颈动脉内膜中层厚度(CIMT)相关,但与年龄、性别、收缩压(SBP)、血脂水平、吸烟和糖尿病等传统 CVD 危险因素无关。我们进行了多阶段分析,该分析基于对接受 ART 治疗超过 6 个月、年龄>45 岁的 HIV 感染患者 CVD 风险的横断面研究。本分析的目的是确定 HIV-1 感染成年人 CIMT 的候选细胞和血浆生物标志物。我们还试图确定这些候选生物标志物是否与之前在 HIV 阴性成年人中确定的传统 CVD 危险因素无关。使用高分辨率 B 型超声图像获得右侧颈总动脉(CCA)的图像。检测了血浆可溶性炎症介质、细胞因子和趋化因子。通过 CD14/CD16 表达定义单核细胞,通过 CD38/HLA-DR 表达定义 CD8+T 细胞活化。受试者的中位年龄为 49.5 岁,87%为男性,CIMT 为 0.73mm,FRS 为 6%,中位病毒载量为 48 拷贝/ml,CD4+T 细胞计数为 479 个/μL。可溶性 VCAM-1 和 CD14dimCD16-单核细胞的扩增均与 CIMT 独立相关,与年龄和 SBP 无关。这些因素是共同动脉粥样硬化过程的不同组成部分;1)血管内皮分子表达和 2)进入血管内皮并促进动脉粥样硬化斑块形成的血管单核细胞。