Division of Vascular Surgery, University of Missouri, School of Medicine, Columbia, Mo.
Department of Health Management and Informatics, University of Missouri, School of Medicine, Columbia, Mo.
J Vasc Surg. 2014 May;59(5):1323-30.e1. doi: 10.1016/j.jvs.2013.11.076. Epub 2014 Jan 7.
The ability of nursing home residents to function independently is associated with their quality of life. The impact of amputations on functional status in this population remains unclear. This analysis evaluated the effect of amputations-transmetatarsal (TM), below-knee (BK), and above-knee (AK)--on the ability of residents to perform self-care activities.
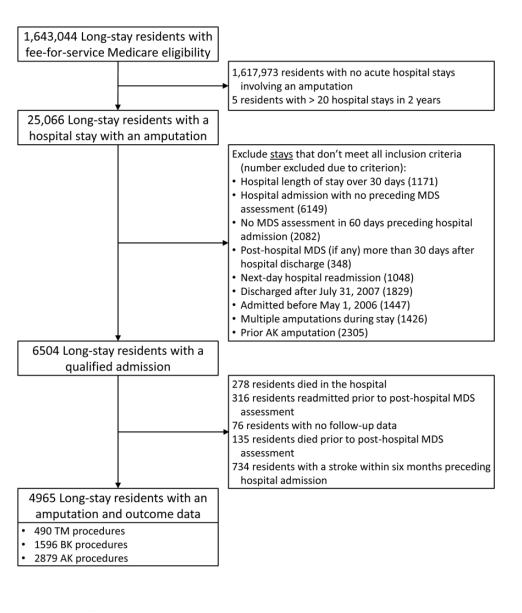
Medicare inpatient claims were linked with nursing home assessment data to identify admissions for amputation. The Minimum Data Set Activities of Daily Living Long Form Score (0-28; higher numbers indicating greater impairment), based on seven activities of daily living, was calculated before and after amputation. Hierarchical modeling determined the effect of the surgery on postamputation function of residents. Controlling for comorbidity, cognition, and prehospital function allowed for evaluation of Activities of Daily Living trajectories over time.
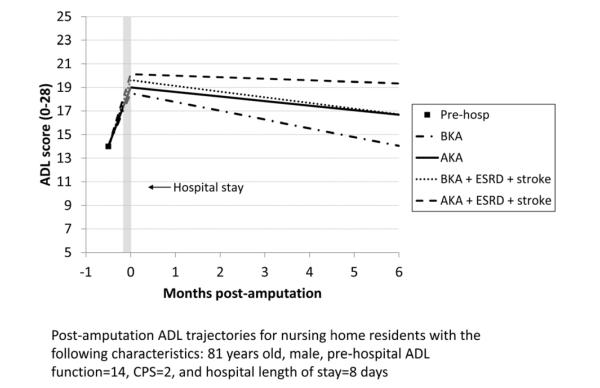
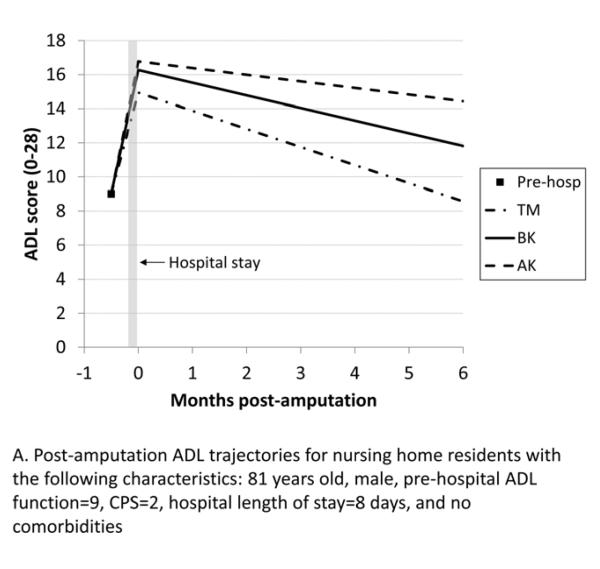
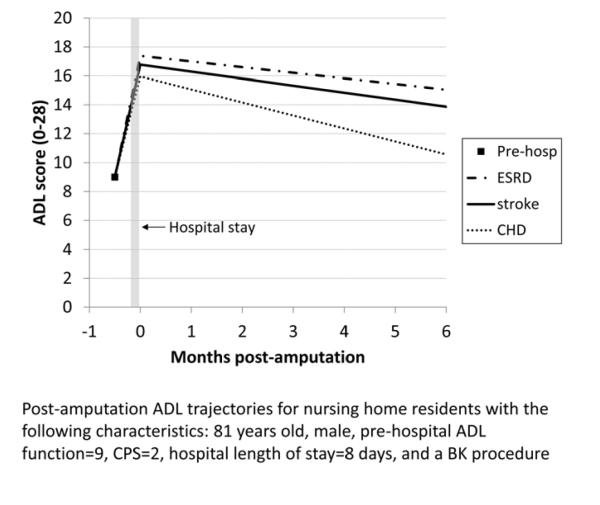
In total, 4965 residents underwent amputation: 490 TM, 1596 BK, and 2879 AK. Mean age was 81 years, and 54% of the patients were women. Most were white (67%) or black (26.5%). Comorbidities before amputation included diabetes mellitus (70.7%), coronary heart disease (57.1%), chronic kidney disease (53.6%), and/or congestive heart failure (52.1%). Mortality within 30 days of hospital discharge was 9.0%, and hospital readmission was 27.7%. Stroke, end-stage renal disease, and poor baseline cognitive function were associated with the poorest functional outcome after amputation. Compared with residents who received TM amputation, those who had BK or AK amputation recovered more slowly and failed to return to baseline function by 6 months. BK was found to have a superior functional trajectory compared with AK.
Elderly nursing home residents undergoing BK or AK amputation failed to return to their functional baseline within 6 months. Among frail elderly nursing home residents, higher amputation level, stroke, end-stage renal disease, poor baseline cognitive scores, and female sex were associated with inferior functional status after amputation. These factors should be strongly assessed to maintain activities of daily living and quality of life in the nursing home population.
养老院居民的独立功能能力与其生活质量相关。截肢对该人群的功能状态的影响尚不清楚。本分析评估了居民进行自我护理活动的能力受截肢(经跖骨、膝下和膝上)的影响。
将医疗保险住院索赔与养老院评估数据相联系,以确定截肢的入院情况。根据七项日常生活活动计算最低数据组日常生活活动长期评分(0-28;分数越高表示损伤越严重),并在截肢前后进行计算。分层模型确定手术对居民截肢后功能的影响。控制合并症、认知和住院前功能,可评估随时间推移的日常生活活动轨迹。
共有 4965 名居民接受了截肢手术:490 例经跖骨、1596 例膝下和 2879 例膝上。平均年龄为 81 岁,54%的患者为女性。大多数为白人(67%)或黑人(26.5%)。截肢前的合并症包括糖尿病(70.7%)、冠心病(57.1%)、慢性肾脏病(53.6%)和/或充血性心力衰竭(52.1%)。出院后 30 天内死亡率为 9.0%,住院再入院率为 27.7%。中风、终末期肾病和认知功能较差基线与截肢后功能最差的结果相关。与接受经跖骨截肢的居民相比,接受膝下或膝上截肢的居民恢复较慢,并且在 6 个月内无法恢复到基线功能。膝下截肢的功能轨迹优于膝上截肢。
在 6 个月内,接受膝下或膝上截肢的老年养老院居民无法恢复其功能基线。在体弱的老年养老院居民中,较高的截肢水平、中风、终末期肾病、较差的认知评分基线和女性与截肢后功能状态较差相关。这些因素应进行严格评估,以维持养老院人群的日常生活活动和生活质量。