Department of Microbiology, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia.
BMC Infect Dis. 2014 Jan 14;14:28. doi: 10.1186/1471-2334-14-28.
Introduction of antiretroviral therapy (ART) in sub-Saharan Africa was a hot debate due to many concerns about adherence, logistics and resistance. Currently, it has been significantly scaled up. However as the WHO clinico-immunological approaches for initiation and monitoring of ART in the region lacks viral load determination and drug resistance monitoring, HIV infected adults and children may be at risk for "unrecognized" virologic failure and the subsequent development of antiretroviral drug resistance. This study evaluates the virological efficacy and immunological recovery of HIV/AIDS patients under ART.
Consecutive HIV-1 infected adults (N = 100) and children (N = 100) who have been receiving ART for up to 6 years at Gondar University Hospital, Ethiopia were enrolled following the WHO protocol for assessment of acquired drug resistance. Magnitude of viral suppression, genotypic drug resistance mutations and patterns of CD4+ T cell recovery were determined using standard virological and immunological methods.
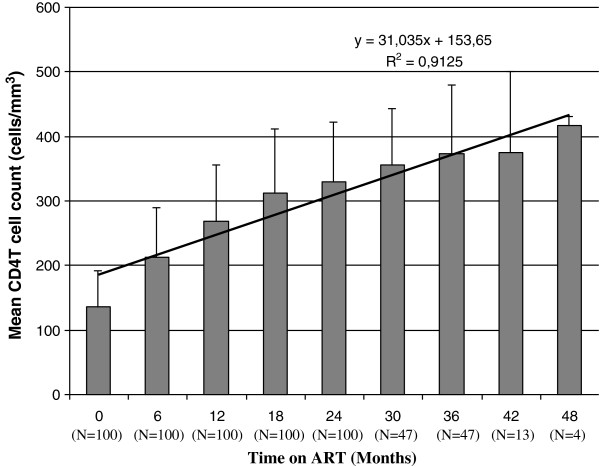
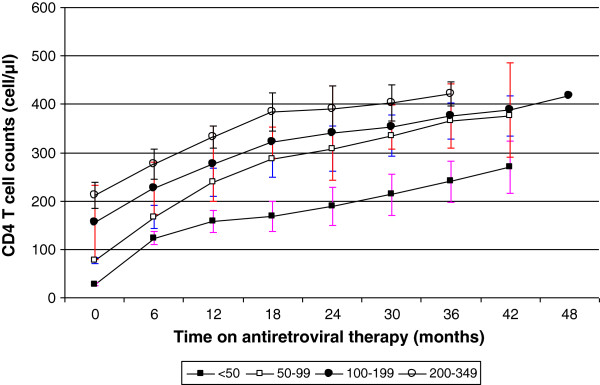
Virological suppression (HIV RNA < 40 copies/ml) was observed in 82 and 87% of adults and children on a median time of 24 months on ART, respectively. Mutation K103N conferring resistance to non nucleoside reverse transcriptase inhibitors and thymidine analogue mutations (M41L, L210W) were found only in one adult and child patient, respectively. Median CD4+ T cell count has increased from baseline 124 to 266 (IQR: 203-306) and 345 (IQR: 17-1435) to 998 (IQR: 678-2205) cells/mm3 in adults and children respectively after 12 months of ART. Nevertheless, small but significant number of clinically asymptomatic adults (16%) and children (13%) had low level viraemia (HIV-1 RNA 41-1000 copies/ml).
Majority of both adults (82%) and children (87%) who received ART showed high viral suppression and immunological recovery. This indicates that despite limited resources in the setting virological efficacy can be sustained for a substantial length of time and also enhance immunological recovery irrespective of age. However, the presence of drug resistance mutations and low level viraemia among clinically asymptomatic patients highlights the need for virological monitoring.
在撒哈拉以南非洲引入抗逆转录病毒疗法(ART)是一个热点争议,因为人们对依从性、后勤保障和耐药性存在诸多担忧。目前,该疗法已得到显著推广。然而,由于世卫组织在该地区启动和监测抗逆转录病毒治疗的临床免疫学方法缺乏病毒载量测定和耐药性监测,HIV 感染者可能面临“未被识别”的病毒学失败和随后的抗逆转录病毒药物耐药性发展风险。本研究评估了接受 ART 治疗的 HIV/AIDS 患者的病毒学疗效和免疫恢复情况。
我们按照世卫组织评估获得性耐药性的方案,连续纳入了在埃塞俄比亚贡德尔大学医院接受 ART 治疗长达 6 年的 100 例 HIV-1 感染成人和 100 例儿童患者。使用标准病毒学和免疫学方法,评估病毒抑制程度、基因型耐药突变情况和 CD4+T 细胞恢复模式。
在中位时间为 24 个月的 ART 治疗后,成人和儿童患者的病毒学抑制率(HIV RNA<40 拷贝/ml)分别为 82%和 87%。仅在一名成人和儿童患者中发现了对非核苷类逆转录酶抑制剂耐药的 K103N 突变和胸苷类似物突变(M41L、L210W)。成人和儿童患者的 CD4+T 细胞计数中位数分别从基线的 124 个/μl 增加到治疗后 12 个月的 266 个/μl(IQR:203-306)和 345 个/μl(IQR:17-1435)、998 个/μl(IQR:678-2205)。尽管如此,仍有相当数量的无症状成人(16%)和儿童(13%)出现低水平病毒血症(HIV-1 RNA 41-1000 拷贝/ml)。
大多数接受 ART 治疗的成人(82%)和儿童(87%)均表现出高病毒抑制和免疫恢复。这表明,尽管资源有限,病毒学疗效仍能在相当长的时间内得以维持,并且无论年龄大小,均可增强免疫恢复。然而,在无症状患者中发现耐药突变和低水平病毒血症,突显了进行病毒学监测的必要性。