*The National AIDS and Sexually Transmitted Infection (STI) Control Programme, Ministry of Health, Nairobi, Kenya; †Kenya National Bureau of Statistics, Nairobi, Kenya; ‡National Public Health Laboratory Services, Ministry of Health, Nairobi, Kenya; §The National Council for Population and Development, Nairobi, Kenya; ‖National AIDS Control Council, Nairobi, Kenya; ¶Kenya Medical Research Institute, Nairobi, Kenya; #Global Health Sciences, University of California, San Francisco, San Francisco, CA; **Ministry of Health, Nairobi, Kenya; and ††Division of Global HIV/AIDS, Center for Global Health, US Centers for Disease Control and Prevention, Nairobi, Kenya.
J Acquir Immune Defic Syndr. 2014 May 1;66 Suppl 1(Suppl 1):S13-26. doi: 10.1097/QAI.0000000000000124.
Enhanced HIV surveillance using demographic, behavioral, and biologic data from national surveys can provide information to evaluate and respond to HIV epidemics efficiently.
From October 2012 to February 2013, we conducted a 2-stage cluster sampling survey of persons aged 18 months to 64 years in 9 geographic regions in Kenya. Participants answered questionnaires and provided blood for HIV testing. We estimated HIV prevalence, HIV incidence, described trends in HIV prevalence over the past 5 years, and identified factors associated with HIV infection. This analysis was restricted to persons aged 15-64 years.
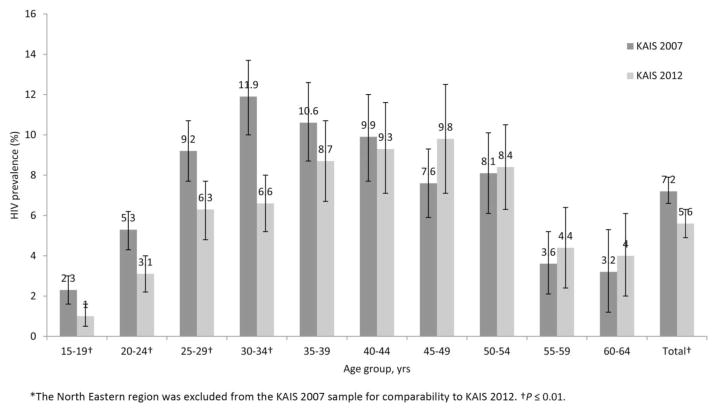
HIV prevalence was 5.6% [95% confidence interval (CI): 4.9 to 6.3] in 2012, a significant decrease from 2007, when HIV prevalence, excluding the North Eastern region, was 7.2% (95% CI: 6.6 to 7.9). HIV incidence was 0.5% (95% CI: 0.2 to 0.9) in 2012. Among women, factors associated with undiagnosed HIV infection included being aged 35-39 years, divorced or separated, from urban residences and Nyanza region, self-perceiving a moderate risk of HIV infection, condom use with the last partner in the previous 12 months, and reporting 4 or more lifetime number of partners. Among men, widowhood, condom use with the last partner in the previous 12 months, and lack of circumcision were associated with undiagnosed HIV infection.
HIV prevalence has declined in Kenya since 2007. With improved access to treatment, HIV prevalence has become more challenging to interpret without data on new infections and mortality. Correlates of undiagnosed HIV infection provide important information on where to prioritize prevention interventions to reduce transmission of HIV in the broader population.
利用来自全国性调查的人口统计学、行为学和生物学数据加强艾滋病毒监测,可以提供信息,以便有效评估和应对艾滋病毒流行。
2012 年 10 月至 2013 年 2 月,我们在肯尼亚 9 个地理区域进行了 2 阶段聚类抽样调查,调查对象为 18 个月至 64 岁的人群。参与者回答了问卷并提供了血液进行艾滋病毒检测。我们估计了艾滋病毒流行率、艾滋病毒发病率,描述了过去 5 年来艾滋病毒流行率的趋势,并确定了与艾滋病毒感染相关的因素。本分析仅限于 15-64 岁的人群。
2012 年艾滋病毒流行率为 5.6%(95%置信区间:4.9%至 6.3%),显著低于 2007 年,当时除东北区域外,艾滋病毒流行率为 7.2%(95%置信区间:6.6%至 7.9%)。2012 年艾滋病毒发病率为 0.5%(95%置信区间:0.2%至 0.9%)。在女性中,与未确诊艾滋病毒感染相关的因素包括年龄在 35-39 岁、离婚或分居、来自城市居住地和奈瓦沙地区、自我感知艾滋病毒感染中度风险、过去 12 个月内与最近性伴侣使用安全套以及报告过去有 4 个或更多性伴侣。在男性中,丧偶、过去 12 个月内与最近性伴侣使用安全套以及未行包皮环切术与未确诊的艾滋病毒感染相关。
自 2007 年以来,肯尼亚的艾滋病毒流行率有所下降。随着治疗机会的增加,如果没有关于新发感染和死亡率的数据,艾滋病毒流行率将更难以解释。未确诊艾滋病毒感染的相关因素为在更广泛的人群中优先开展预防干预措施以减少艾滋病毒传播提供了重要信息。