Department of Anesthesia, St Joseph's Hospital, McMaster University, Hamilton, ON, Canada.
Department of Clinical Epidemiology and Biostatistics, St Joseph's Hospital, McMaster University, Hamilton, ON, Canada.
J Pain Res. 2014 Jan 10;7:47-55. doi: 10.2147/JPR.S55749.
No proof of efficacy, in the form of a randomized controlled trial (RCT), exists to support pulsed radiofrequency (PRF) treatment of the dorsal root ganglion (DRG) for chronic lumbar radicular (CLR) pain. We determined the feasibility of a larger trial (primary objective), and also explored the efficacy of PRF in decreasing pain on a visual analog scale (VAS) and improving the Oswestry Disability Index.
This was a single-center, placebo-controlled, triple-blinded RCT. Patients were randomized to a placebo group (needle placement) or a treatment group (PRF at 42°C for 120 seconds to the DRG). Patients were followed up for 3 months post procedure. Outcomes with regard to pain, Oswestry Disability Index score, and side effects were analyzed on an intention-to-treat basis.
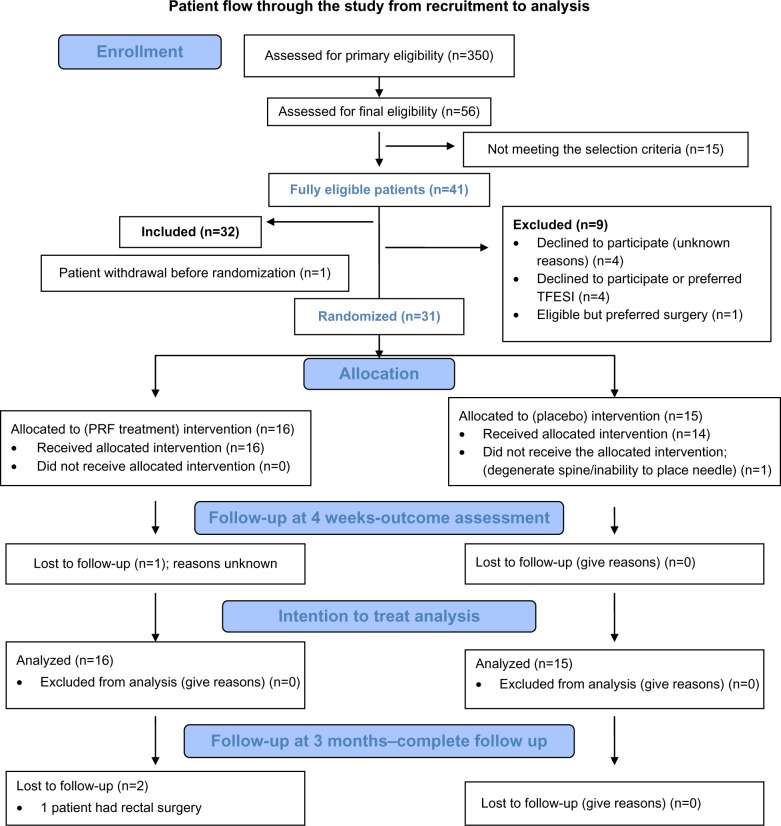
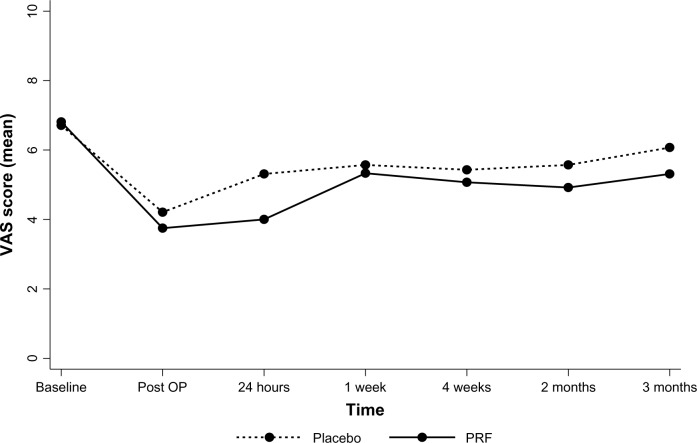
Over 15 months, 350 potential patients were identified and 56 were assessed for eligibility. Fifteen of them did not meet the selection criteria. Of the 41 eligible patients, 32 (78%) were recruited. One patient opted out before intervention. Three patients were lost to follow-up at 3 months. Mean VAS differences were not significantly different at 4 weeks (-0.36, 95% confidence interval [CI], -2.29, 1.57) or at 3 months (-0.76, 95% CI, -3.14, 1.61). The difference in mean Oswestry Disability Index score was also not significantly different at 4 weeks (-2%, 95% CI, -14%, 10%) or 3 months (-7%, 95% CI, -21%, 6%). There were no major side effects. Six of 16 patients in the PRF group and three of 15 in the placebo group showed a >50% decrease in VAS score.
The recruitment rate was partially successful. At 3 months, the relative success of PRF-DRG was small. A large-scale trial to establish efficacy is not practically feasible considering the small effect size, which would necessitate recruitment of a challengingly large number of participants over a number of years. Until clear parameters for application of PRF are established, clinicians will need to use their individual judgment regarding its clinical applicability, given the present evidence.
没有随机对照试验(RCT)的疗效证据支持脉冲射频(PRF)治疗背根神经节(DRG)治疗慢性腰椎神经根性(CLR)疼痛。我们确定了更大规模试验的可行性(主要目标),并探讨了 PRF 降低疼痛视觉模拟量表(VAS)评分和改善 Oswestry 残疾指数的疗效。
这是一项单中心、安慰剂对照、三盲 RCT。患者被随机分配至安慰剂组(针放置)或治疗组(DRG 处 42°C 持续 120 秒的 PRF)。患者在术后 3 个月进行随访。根据意向治疗原则分析疼痛、Oswestry 残疾指数评分和不良反应的结果。
在 15 个月内,确定了 350 名潜在患者,对 56 名患者进行了入选评估。其中 15 名不符合入选标准。在 41 名合格患者中,有 32 名(78%)入选。1 名患者在干预前退出。3 名患者在 3 个月时失访。4 周时 VAS 差值的均值差异无统计学意义(-0.36,95%置信区间 [CI],-2.29,1.57)或 3 个月时(-0.76,95%CI,-3.14,1.61)。4 周和 3 个月时 Oswestry 残疾指数评分差值的均值差异也无统计学意义(-2%,95%CI,-14%,10%)或(-7%,95%CI,-21%,6%)。无重大不良反应。16 名 PRF 组患者中有 6 名和 15 名安慰剂组患者中有 3 名 VAS 评分下降超过 50%。
招募率部分成功。3 个月时,PRF-DRG 的相对疗效较小。考虑到效应量较小,进行大规模试验以确定疗效在实践上是不可行的,这将需要在数年时间内招募大量参与者。在明确 PRF 应用的参数之前,鉴于目前的证据,临床医生需要根据其个体判断来确定其临床适用性。