Lofters Aisha, Slater Morgan, Kirst Maritt, Shankardass Ketan, Quiñonez Carlos
Centre for Research on Inner City Health, St. Michael's Hospital, Toronto, Ontario, Canada ; St. Michael's Department of Family & Community Medicine, University of Toronto, Toronto, Ontario, Canada.
St. Michael's Department of Family & Community Medicine, University of Toronto, Toronto, Ontario, Canada.
PLoS One. 2014 Jan 13;9(1):e85286. doi: 10.1371/journal.pone.0085286. eCollection 2014.
Substantive equity-focused policy changes in Ontario, Canada have yet to be realized and may be limited by a lack of widespread public support. An understanding of how the public attributes inequalities can be informative for developing widespread support. Therefore, the objectives of this study were to examine how Ontarians attribute income-related health inequalities.
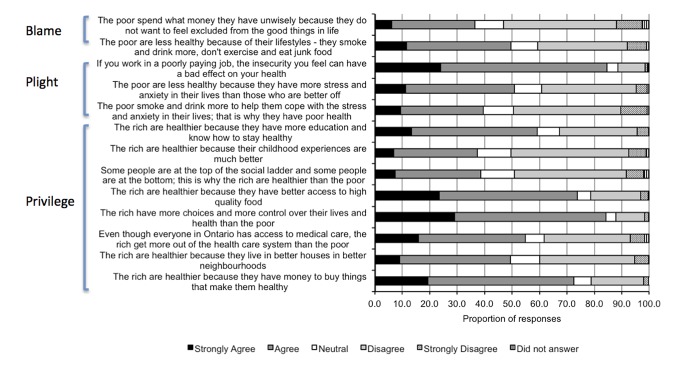
We conducted a telephone survey of 2,006 Ontarians using random digit dialing. The survey included thirteen questions relevant to the theme of attributions of income-related health inequalities, with each statement linked to a known social determinant of health. The statements were further categorized depending on whether the statement was framed around blaming the poor for health inequalities, the plight of the poor as a cause of health inequalities, or the privilege of the rich as a cause of health inequalities.
There was high agreement for statements that attributed inequalities to differences between the rich and the poor in terms of employment, social status, income and food security, and conversely, the least agreement for statements that attributed inequalities to differences in terms of early childhood development, social exclusion, the social gradient and personal health practices and coping skills. Mean agreement was lower for the two statements that suggested blame for income-related health inequalities lies with the poor (43.1%) than for the three statements that attributed inequalities to the plight of the poor (58.3%) or the eight statements that attributed inequalities to the privilege of the rich (58.7%).
A majority of this sample of Ontarians were willing to attribute inequalities to the social determinants of health, and were willing to accept messages that framed inequalities around the privilege of the rich or the plight of the poor. These findings will inform education campaigns, campaigns aimed at increasing public support for equity-focused public policy, and knowledge translation strategies.
加拿大安大略省尚未实现以实质性公平为重点的政策变革,可能会因缺乏广泛的公众支持而受到限制。了解公众如何归因不平等现象,对于获得广泛支持可能具有指导意义。因此,本研究的目的是调查安大略省居民如何归因与收入相关的健康不平等现象。
我们使用随机数字拨号对2006名安大略省居民进行了电话调查。该调查包括13个与收入相关的健康不平等归因主题相关的问题,每个陈述都与一个已知的健康社会决定因素相关。这些陈述根据是否围绕将健康不平等归咎于穷人、穷人的困境是健康不平等的原因,还是富人的特权是健康不平等的原因进行了进一步分类。
对于将不平等归因于富人和穷人在就业、社会地位、收入和粮食安全方面的差异的陈述,人们的认可度很高;相反,对于将不平等归因于儿童早期发展、社会排斥、社会梯度以及个人健康行为和应对技能方面的差异的陈述,认可度最低。对于暗示将与收入相关的健康不平等归咎于穷人的两个陈述(43.1%),平均认可度低于将不平等归因于穷人困境的三个陈述(58.3%)或归因于富人特权的八个陈述(58.7%)。
这个安大略省居民样本中的大多数人愿意将不平等归因于健康的社会决定因素,并愿意接受围绕富人特权或穷人困境来阐述不平等的信息。这些发现将为教育活动、旨在增加公众对以公平为重点的公共政策支持的活动以及知识转化策略提供参考。