Centre for Orthopaedic and Trauma Research, The University of Adelaide, Royal Adelaide Hospital, Level 4 Bice Building, Adelaide, South Australia, 5000, Australia,
Curr Osteoporos Rep. 2014 Mar;12(1):127-34. doi: 10.1007/s11914-014-0192-5.
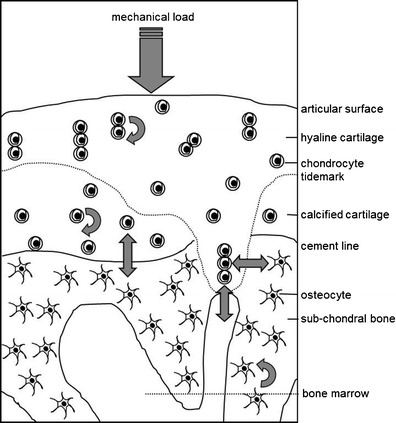
There is now general agreement that osteoarthritis (OA) involves all structures in the affected joint, culminating in the degradation of the articular cartilage. It is appropriate to focus particularly on the subchondral bone because characteristic changes occur in this tissue with disease progression, either in parallel, or contributing to, the loss of cartilage volume and quality. Changes in both the articular cartilage and the subchondral bone are mediated by the cells in these two compartments, chondrocytes and cells of the osteoblast lineage, respectively, whose primary roles are to maintain the integrity and function of these tissues. In addition, altered rates of bone remodeling across the disease process are due to increased or decreased osteoclastic bone resorption. In the altered mechanical and biochemical environment of a progressively diseased joint, the cells function differently and show a different profile of gene expression, suggesting direct effects of these external influences. There is also ex vivo and in vitro evidence of chemical crosstalk between the cells in cartilage and subchondral bone, suggesting an interdependence of events in the two compartments and therefore indirect effects of, for example, altered loading of the joint. It is ultimately these cellular changes that explain the altered morphology of the cartilage and subchondral bone. With respect to crosstalk between the cells in cartilage and bone, there is evidence that small molecules can transit between these tissues. For larger molecules, such as inflammatory mediators, this is an intriguing possibility but remains to be demonstrated. The cellular changes during the progression of OA almost certainly need to be considered in a temporal and spatial manner, since it is important when and where observations are made in either human disease or animal models of OA. Until recently, comparisons have been made with the assumption, for example, that the subchondral bone is behaviorally uniform, but this is not the case in OA, where regional differences of the bone are evident using magnetic resonance imaging (MRI). Nevertheless, an appreciation of the altered cell function during the progression of OA will identify new disease modifying targets. If, indeed, the cartilage and subchondral bone behave as an interconnected functional unit, normalization of cell behavior in one compartment may have benefits in both tissues.
现在普遍认为骨关节炎(OA)涉及受影响关节的所有结构,最终导致关节软骨退化。特别关注软骨下骨是恰当的,因为随着疾病的进展,该组织会出现特征性变化,这些变化要么与软骨体积和质量的丧失平行,要么导致其丧失。关节软骨和软骨下骨的变化都是由这两个隔室中的细胞介导的,分别是软骨细胞和成骨细胞谱系的细胞,它们的主要作用是维持这些组织的完整性和功能。此外,在疾病过程中,由于破骨细胞骨吸收的增加或减少,骨重塑的速度发生改变。在一个逐渐患病的关节的改变的力学和生化环境中,细胞的功能不同,表现出不同的基因表达谱,这表明这些外部影响有直接作用。还有离体和体外证据表明软骨和软骨下骨细胞之间存在化学串扰,这表明两个隔室中的事件相互依赖,因此关节负荷改变等间接影响。正是这些细胞变化解释了软骨和软骨下骨形态的改变。关于软骨和骨细胞之间的串扰,有证据表明小分子可以在这些组织之间转移。对于较大的分子,如炎症介质,这是一个有趣的可能性,但仍有待证明。OA 进展过程中的细胞变化几乎肯定需要以时间和空间的方式来考虑,因为在观察人类疾病或 OA 动物模型时,何时何地观察到这些变化非常重要。直到最近,人们还一直假设软骨下骨的行为是均匀的,例如,进行比较,但在 OA 中并非如此,通过磁共振成像(MRI)可以明显看出骨的区域性差异。然而,对 OA 进展过程中细胞功能改变的认识将确定新的疾病修饰靶点。如果软骨和软骨下骨确实表现为相互关联的功能单元,那么一个隔室中细胞功能的正常化可能会对两个组织都有益。