Payne Beth A, Hutcheon Jennifer A, Ansermino J Mark, Hall David R, Bhutta Zulfiqar A, Bhutta Shereen Z, Biryabarema Christine, Grobman William A, Groen Henk, Haniff Farizah, Li Jing, Magee Laura A, Merialdi Mario, Nakimuli Annettee, Qu Ziguang, Sikandar Rozina, Sass Nelson, Sawchuck Diane, Steyn D Wilhelm, Widmer Mariana, Zhou Jian, von Dadelszen Peter
Department of Obstetrics and Gynaecology and the CFRI Reproductive and Healthy Pregnancy Cluster, University of British Columbia, Vancouver, Canada.
Department of Obstetrics and Gynaecology and the CFRI Reproductive and Healthy Pregnancy Cluster, University of British Columbia, Vancouver, Canada ; School of Population and Public Health, University of British Columbia, Vancouver, Canada.
PLoS Med. 2014 Jan;11(1):e1001589. doi: 10.1371/journal.pmed.1001589. Epub 2014 Jan 21.
Pre-eclampsia/eclampsia are leading causes of maternal mortality and morbidity, particularly in low- and middle- income countries (LMICs). We developed the miniPIERS risk prediction model to provide a simple, evidence-based tool to identify pregnant women in LMICs at increased risk of death or major hypertensive-related complications.
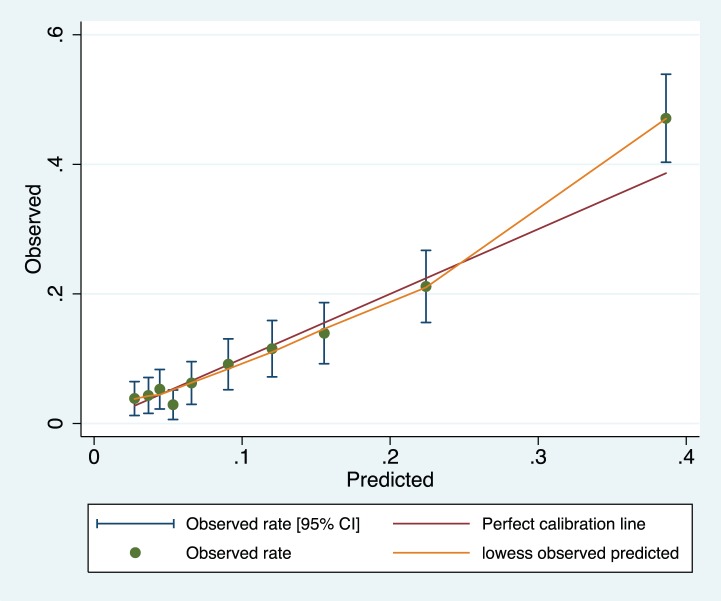
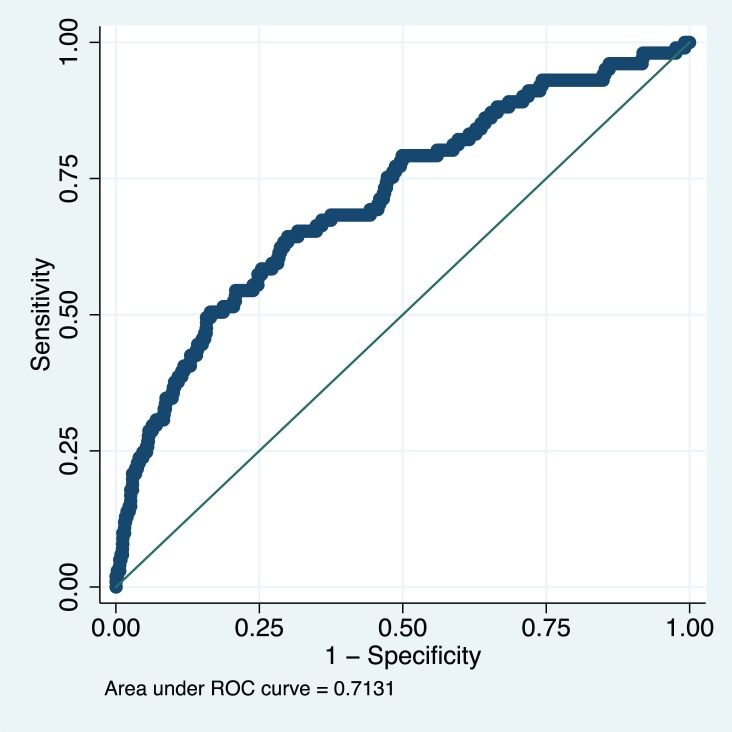
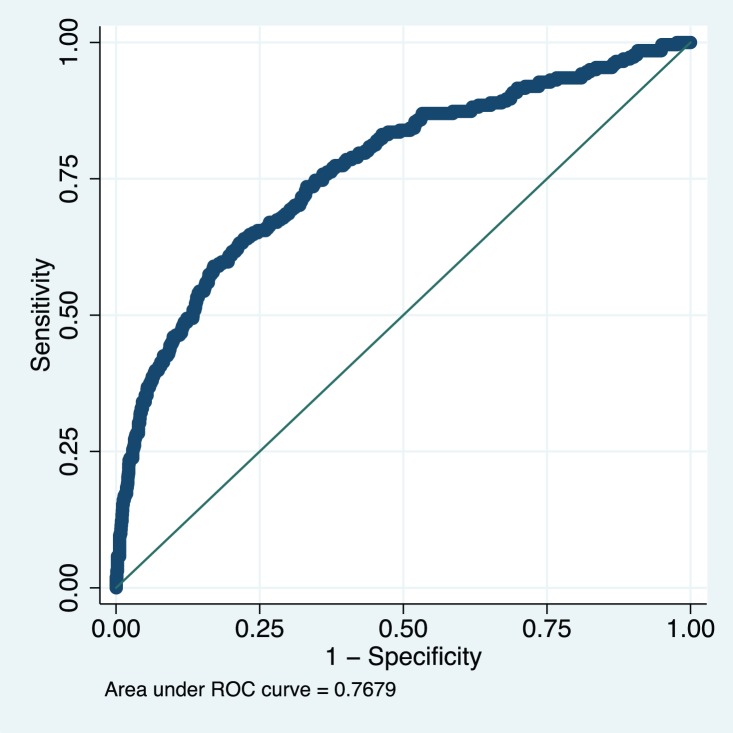
From 1 July 2008 to 31 March 2012, in five LMICs, data were collected prospectively on 2,081 women with any hypertensive disorder of pregnancy admitted to a participating centre. Candidate predictors collected within 24 hours of admission were entered into a step-wise backward elimination logistic regression model to predict a composite adverse maternal outcome within 48 hours of admission. Model internal validation was accomplished by bootstrapping and external validation was completed using data from 1,300 women in the Pre-eclampsia Integrated Estimate of RiSk (fullPIERS) dataset. Predictive performance was assessed for calibration, discrimination, and stratification capacity. The final miniPIERS model included: parity (nulliparous versus multiparous); gestational age on admission; headache/visual disturbances; chest pain/dyspnoea; vaginal bleeding with abdominal pain; systolic blood pressure; and dipstick proteinuria. The miniPIERS model was well-calibrated and had an area under the receiver operating characteristic curve (AUC ROC) of 0.768 (95% CI 0.735-0.801) with an average optimism of 0.037. External validation AUC ROC was 0.713 (95% CI 0.658-0.768). A predicted probability ≥25% to define a positive test classified women with 85.5% accuracy. Limitations of this study include the composite outcome and the broad inclusion criteria of any hypertensive disorder of pregnancy. This broad approach was used to optimize model generalizability.
The miniPIERS model shows reasonable ability to identify women at increased risk of adverse maternal outcomes associated with the hypertensive disorders of pregnancy. It could be used in LMICs to identify women who would benefit most from interventions such as magnesium sulphate, antihypertensives, or transportation to a higher level of care.
先兆子痫/子痫是孕产妇发病和死亡的主要原因,在低收入和中等收入国家(LMICs)尤为如此。我们开发了miniPIERS风险预测模型,以提供一种简单的、基于证据的工具,用于识别LMICs中死亡风险或主要高血压相关并发症风险增加的孕妇。
2008年7月1日至2012年3月31日期间,在5个LMICs中,前瞻性收集了2081名入住参与中心的患有任何妊娠高血压疾病的妇女的数据。将入院24小时内收集的候选预测因素纳入逐步向后排除逻辑回归模型,以预测入院48小时内的综合不良孕产妇结局。模型内部验证通过自抽样法完成,外部验证使用先兆子痫风险综合评估(fullPIERS)数据集中1300名妇女的数据完成。对校准、区分和分层能力进行预测性能评估。最终的miniPIERS模型包括:产次(初产妇与经产妇);入院时的孕周;头痛/视觉障碍;胸痛/呼吸困难;伴有腹痛的阴道出血;收缩压;以及试纸法蛋白尿。miniPIERS模型校准良好,受试者工作特征曲线下面积(AUC ROC)为(0.768)((95%)CI (0.735 - 0.801)),平均乐观度为(0.037)。外部验证AUC ROC为(0.713)((95%)CI (0.658 - 0.768))。预测概率≥(25%)定义为阳性检测,对妇女分类的准确率为(85.5%)。本研究的局限性包括综合结局以及任何妊娠高血压疾病的广泛纳入标准。采用这种广泛的方法是为了优化模型的通用性。
miniPIERS模型显示出合理的能力,能够识别与妊娠高血压疾病相关的不良孕产妇结局风险增加的妇女。它可用于LMICs中识别那些将从硫酸镁、抗高血压药物或转运至更高水平医疗护理等干预措施中获益最大的妇女。