Korkes Ilana Levy, Schvartsman Gustavo, Lizuka Ilson Jorge, Quinto Beata Marie, Dalboni Maria Aparecida, Canziani Maria Eugênia, Draibe Sergio Antonio, Pereira Virgilio Gonçalves, Santos Bento Fortunato Cardoso Dos, Monte Julio Cesar Martins, Durão Junior Marcelino de Souza, Batista Marcelo Costa, Santos Oscar Fernando Pavão Dos, Góes Junior Miguel Angelo de, Cendoroglo Neto Miguel
Einstein (Sao Paulo). 2013 Dec;11(4):472-8. doi: 10.1590/s1679-45082013000400012.
To investigate the relation between the need for red blood cell transfusion and serum levels of soluble-Fas, erythropoietin and inflammatory cytokines in critically ill patients with and without acute kidney injury.
We studied critically ill patients with acute kidney injury (n=30) and without acute kidney injury (n=13), end-stage renal disease patients on hemodialysis (n=25) and healthy subjects (n=21). Serum levels of soluble-Fas, erythropoietin, interleukin 6, interleukin 10, iron status, hemoglobin and hematocrit concentration were analyzed in all groups. The association between these variables in critically ill patients was investigated.
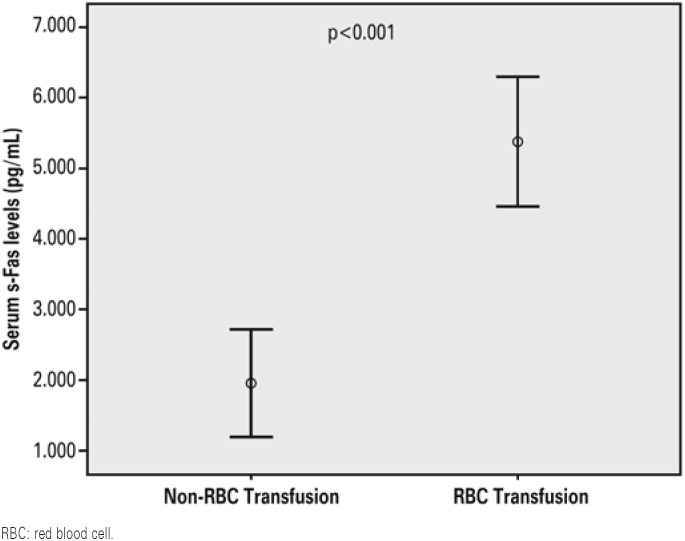
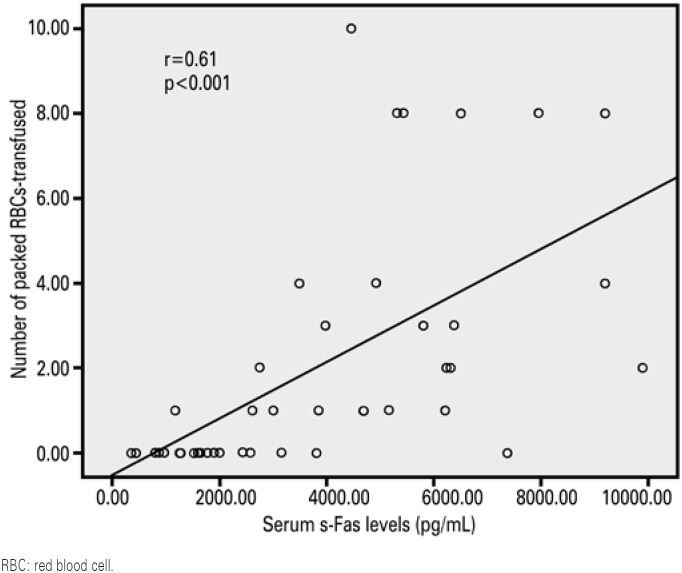
Critically ill patients (acute kidney injury and non-acute kidney injury patients) had higher serum levels of erythropoietin than the other groups. Hemoglobin concentration was lower in the acute kidney injury patients than in other groups. Serum soluble-Fas levels were higher in acute kidney injury and end-stage renal disease patients. Critically ill patients requiring red blood cell transfusions had higher serum levels of soluble-Fas (5,906±2,047 and 1,920±1,060; p<0.001), interleukin 6 (518±537 and 255+502; p=0.02) and interleukin 10 (35.8±30.7 and 18.5±10.9; p=0.02), better iron status and higher mortality rates in the first 28 days in intensive care unit. Serum soluble-Fas levels were independently associated with the number of red blood cell units transfused (p=0.02). Serum soluble-Fas behaved as an independent predictor of the need for red blood cell transfusion in critically ill patients (p=0.01).
Serum soluble-Fas level is an independent predictor of the need for red blood cell transfusion in critically ill patients with or without acute kidney injury. Further studies are warranted to reconfirm this finding.
探讨合并或未合并急性肾损伤的重症患者红细胞输血需求与血清可溶性Fas、促红细胞生成素及炎性细胞因子水平之间的关系。
我们研究了合并急性肾损伤的重症患者(n = 30)、未合并急性肾损伤的重症患者(n = 13)、接受血液透析的终末期肾病患者(n = 25)以及健康受试者(n = 21)。分析了所有组别的血清可溶性Fas、促红细胞生成素、白细胞介素6、白细胞介素10、铁状态、血红蛋白和血细胞比容浓度。研究了重症患者中这些变量之间的关联。
重症患者(急性肾损伤和非急性肾损伤患者)的血清促红细胞生成素水平高于其他组。急性肾损伤患者的血红蛋白浓度低于其他组。急性肾损伤和终末期肾病患者的血清可溶性Fas水平较高。需要红细胞输血的重症患者血清可溶性Fas水平(5906±2047和1920±1060;p<0.001)、白细胞介素6水平(518±537和255 + 502;p = 0.02)和白细胞介素10水平(35.8±30.7和18.5±10.9;p = 0.02)更高,铁状态更好,在重症监护病房的前28天死亡率更高。血清可溶性Fas水平与输注红细胞单位数量独立相关(p = 0.02)。血清可溶性Fas是重症患者红细胞输血需求的独立预测指标(p = 0.01)。
血清可溶性Fas水平是合并或未合并急性肾损伤的重症患者红细胞输血需求的独立预测指标。有必要进行进一步研究以再次证实这一发现。