Poukkanen Meri, Koskenkari Juha, Vaara Suvi T, Pettilä Ville, Karlsson Sari, Korhonen Anna-Maija, Laurila Jouko J, Kaukonen Kirsi-Maija, Lund Vesa, Ala-Kokko Tero I
Crit Care. 2014 Feb 5;18(1):R26. doi: 10.1186/cc13716.
Indications for renal replacement therapy (RRT) have not been generally standardized and vary among intensive care units (ICUs). We aimed to assess the proportion, indications, and modality of RRT, as well as the association between the proportion of RRT use and 90-day mortality in patients with septic shock in Finnish adult ICUs.
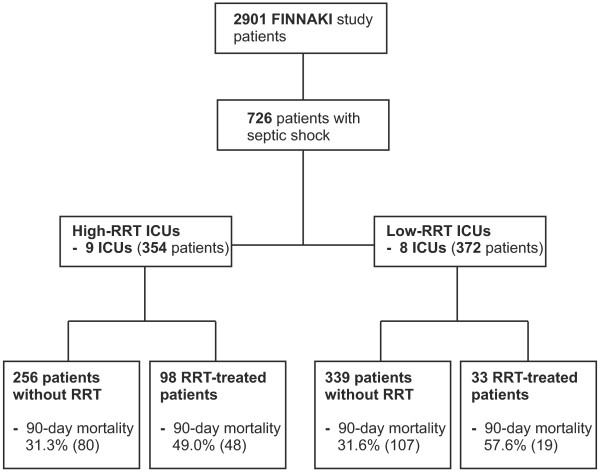
We identified patients with septic shock from the prospective observational multicenter FINNAKI study conducted between 1 September 2011 and 1 February 2012. We divided the ICUs into high-RRT and low-RRT ICUs according to the median of the proportion of RRT-treated patients with septic shock. Differences in indications, and modality of RRT between ICU groups were assessed. Finally, we performed an adjusted logistic regression analysis to evaluate the possible association of the ICU group (high vs. low-RRT) with 90-day mortality.
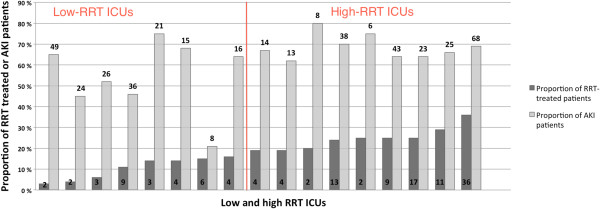
Of the 726 patients with septic shock, 131 (18.0%, 95% CI 15.2 to 20.9%) were treated with RRT. The proportion of RRT-treated patients varied from 3% up to 36% (median 19%) among ICUs. High-RRT ICUs included nine ICUs (354 patients) and low-RRT ICUs eight ICUs (372 patients). In the high-RRT ICUs patients with septic shock were older (P = 0.04), had more cardiovascular (P <0.001) and renal failures (P = 0.003) on the first day in the ICU, were more often mechanically ventilated, and received higher maximum doses of norepinephrine (0.25 μg/kg/min vs. 0.18 μg/kg/min, P <0.001) than in the low-RRT ICUs. No significant differences in indications for or modality of RRT existed between the ICU groups. The crude 90-day mortality rate for patients with septic shock was 36.2% (95% CI 31.1 to 41.3%) in the high-RRT ICUs compared to 33.9% (95% CI 29.0 to 38.8%) in the low-RRT ICUs, P = 0.5. In an adjusted logistic regression analysis the ICU group (high-RRT or low-RRT ICUs) was not associated with 90-day mortality.
Patients with septic shock in ICUs with a high proportion of RRT had more severe organ dysfunctions and received more organ-supportive treatments. Importantly, the ICU group (high-RRT or low-RRT group) was not associated with 90-day mortality.
肾脏替代治疗(RRT)的指征尚未普遍标准化,在重症监护病房(ICU)之间存在差异。我们旨在评估芬兰成人ICU中感染性休克患者接受RRT的比例、指征和方式,以及RRT使用比例与90天死亡率之间的关联。
我们从2011年9月1日至2012年2月1日进行的前瞻性观察性多中心FINNAKI研究中识别出感染性休克患者。我们根据接受RRT治疗的感染性休克患者比例的中位数,将ICU分为高RRT和低RRT的ICU。评估了ICU组之间RRT的指征和方式的差异。最后,我们进行了调整后的逻辑回归分析,以评估ICU组(高RRT与低RRT)与90天死亡率之间的可能关联。
在726例感染性休克患者中,131例(18.0%,95%CI 15.2至20.9%)接受了RRT治疗。各ICU中接受RRT治疗的患者比例从3%到36%不等(中位数为19%)。高RRT的ICU包括9个ICU(354例患者),低RRT的ICU包括8个ICU(372例患者)。在高RRT的ICU中,感染性休克患者年龄更大(P = 0.04),入住ICU第一天时心血管功能不全(P <0.001)和肾衰竭(P = 0.003)更多,机械通气更频繁,接受去甲肾上腺素的最大剂量更高(0.25μg/kg/min对0.18μg/kg/min,P <0.001),高于低RRT的ICU。ICU组之间RRT的指征或方式没有显著差异。高RRT的ICU中感染性休克患者的90天粗死亡率为36.2%(95%CI 31.1至41.3%),而低RRT的ICU中为33.9%(95%CI 29.0至38.8%),P = 0.5。在调整后的逻辑回归分析中,ICU组(高RRT或低RRT的ICU)与90天死亡率无关。
RRT比例高的ICU中感染性休克患者的器官功能障碍更严重,接受的器官支持治疗更多。重要的是,ICU组(高RRT或低RRT组)与90天死亡率无关。