Vaara Suvi T, Korhonen Anna-Maija, Kaukonen Kirsi-Maija, Nisula Sara, Inkinen Outi, Hoppu Sanna, Laurila Jouko J, Mildh Leena, Reinikainen Matti, Lund Vesa, Parviainen Ilkka, Pettilä Ville
Crit Care. 2012 Oct 17;16(5):R197. doi: 10.1186/cc11682.
Positive fluid balance has been associated with an increased risk for mortality in critically ill patients with acute kidney injury with or without renal replacement therapy (RRT). Data on fluid accumulation prior to RRT initiation and mortality are limited. We aimed to study the association between fluid accumulation at RRT initiation and 90-day mortality.
We conducted a prospective, multicenter, observational cohort study in 17 Finnish intensive care units (ICUs) during a five-month period. We collected data on patient characteristics, RRT timing, and parameters at RRT initiation. We studied the association of parameters at RRT initiation, including fluid overload (defined as cumulative fluid accumulation > 10% of baseline weight) with 90-day mortality.
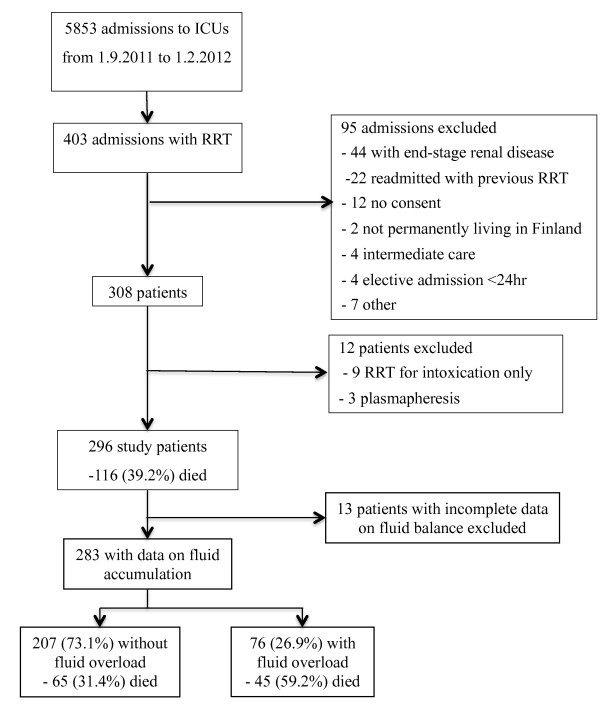
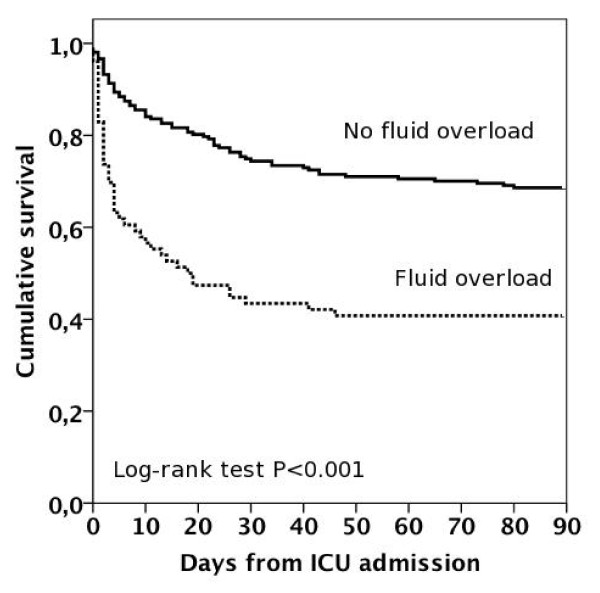
We included 296 RRT-treated critically ill patients. Of 283 patients with complete data on fluid balance, 76 (26.9%) patients had fluid overload. The median (interquartile range) time from ICU admission to RRT initiation was 14 (3.3 to 41.5) hours. The 90-day mortality rate of the whole cohort was 116 of 296 (39.2%; 95% confidence interval 38.6 to 39.8%). The crude 90-day mortality of patients with or without fluid overload was 45 of 76 (59.2%) vs. 65 of 207 (31.4%), P < 0.001. In logistic regression, fluid overload was associated with an increased risk for 90-day mortality (odds ratio 2.6) after adjusting for disease severity, time of RRT initiation, initial RRT modality, and sepsis. Of the 168 survivors with data on RRT use at 90 days, 34 (18.9%, 95% CI 13.2 to 24.6%) were still dependent on RRT.
Patients with fluid overload at RRT initiation had twice as high crude 90-day mortality compared to those without. Fluid overload was associated with increased risk for 90-day mortality even after adjustments.
在接受或未接受肾脏替代治疗(RRT)的急性肾损伤重症患者中,正液体平衡与死亡风险增加相关。关于RRT开始前液体蓄积与死亡率的数据有限。我们旨在研究RRT开始时的液体蓄积与90天死亡率之间的关联。
我们在芬兰的17个重症监护病房(ICU)进行了一项为期5个月的前瞻性、多中心观察性队列研究。我们收集了患者特征、RRT时间以及RRT开始时的参数数据。我们研究了RRT开始时的参数,包括液体超负荷(定义为累积液体蓄积>基线体重的10%)与90天死亡率之间的关联。
我们纳入了296例接受RRT治疗的重症患者。在283例有完整液体平衡数据的患者中,76例(26.9%)患者存在液体超负荷。从ICU入院到开始RRT的中位(四分位间距)时间为14(3.3至41.5)小时。整个队列的90天死亡率为296例中的116例(39.2%;95%置信区间38.6至39.8%)。有或无液体超负荷患者的90天粗死亡率分别为76例中的45例(59.2%)和207例中的65例(31.4%),P<0.001。在逻辑回归中,在调整疾病严重程度、RRT开始时间、初始RRT方式和脓毒症后,液体超负荷与90天死亡风险增加相关(比值比2.6)。在90天时具有RRT使用数据的168例幸存者中,34例(18.9%,95%CI 13.2至24.6%)仍依赖RRT。
RRT开始时存在液体超负荷的患者,其90天粗死亡率是无液体超负荷患者的两倍。即使经过调整,液体超负荷仍与90天死亡风险增加相关。