Wellcome Trust Major Overseas Programme, Oxford University Clinical Research Unit, Hospital for Tropical Diseases, 764 Vo Van Kiet, District 5, Ho Chi Minh City, Vietnam.
BMC Infect Dis. 2014 Feb 10;14:73. doi: 10.1186/1471-2334-14-73.
Typhoid fever is a systemic infection caused by the bacterium Salmonella enterica serovar Typhi. Age, sex, prolonged duration of illness, and infection with an antimicrobial resistant organism have been proposed risk factors for the development of severe disease or fatality in typhoid fever.
We analysed clinical data from 581 patients consecutively admitted with culture confirmed typhoid fever to two hospitals in Vietnam during two periods in 1993-1995 and 1997-1999. These periods spanned a change in the antimicrobial resistance phenotypes of the infecting organisms i.e. fully susceptible to standard antimicrobials, resistance to chloramphenicol, ampicillin and trimethoprim-sulphamethoxazole (multidrug resistant, MDR), and intermediate susceptibility to ciprofloxacin (nalidixic acid resistant). Age, sex, duration of illness prior to admission, hospital location and the presence of MDR or intermediate ciprofloxacin susceptibility in the infecting organism were examined by logistic regression analysis to identify factors independently associated with severe typhoid at the time of hospital admission.
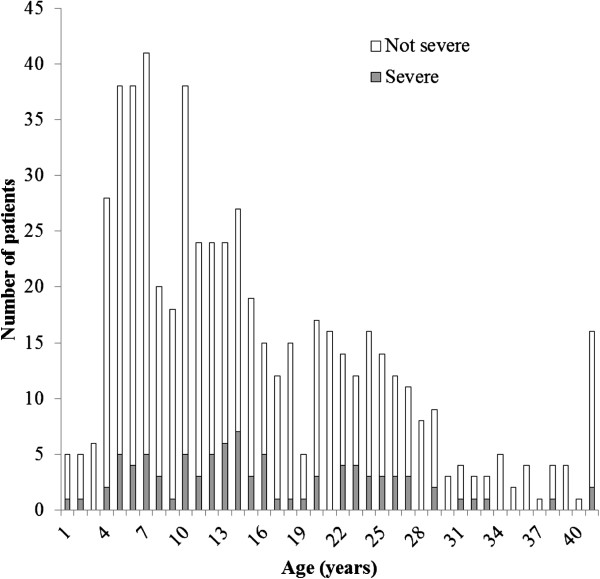
The prevalence of severe typhoid was 15.5% (90/581) and included: gastrointestinal bleeding (43; 7.4%); hepatitis (29; 5.0%); encephalopathy (16; 2.8%); myocarditis (12; 2.1%); intestinal perforation (6; 1.0%); haemodynamic shock (5; 0.9%), and death (3; 0.5%). Severe disease was more common with increasing age, in those with a longer duration of illness and in patients infected with an organism exhibiting intermediate susceptibility to ciprofloxacin. Notably an MDR phenotype was not associated with severe disease. Severe disease was independently associated with infection with an organism with an intermediate susceptibility to ciprofloxacin (AOR 1.90; 95% CI 1.18-3.07; p = 0.009) and male sex (AOR 1.61 (1.00-2.57; p = 0.035).
In this group of patients hospitalised with typhoid fever infection with an organism with intermediate susceptibility to ciprofloxacin was independently associated with disease severity. During this period many patients were being treated with fluoroquinolones prior to hospital admission. Ciprofloxacin and ofloxacin should be used with caution in patients infected with S. Typhi that have intermediate susceptibility to ciprofloxacin.
伤寒是由肠沙门氏菌血清型 Typhi 引起的全身性感染。年龄、性别、疾病持续时间较长以及感染具有抗微生物药物耐药性的生物体被认为是伤寒发生严重疾病或死亡的危险因素。
我们分析了 1993-1995 年和 1997-1999 年期间在越南的两家医院连续收治的 581 例经培养证实的伤寒患者的临床数据。这两个时期跨越了感染生物体的抗微生物药物耐药表型的变化,即对标准抗微生物药物完全敏感、对氯霉素、氨苄西林和甲氧苄啶-磺胺甲噁唑(多药耐药,MDR)耐药以及对环丙沙星(萘啶酸耐药)中介敏感。通过逻辑回归分析检查年龄、性别、入院前疾病持续时间、医院位置以及感染生物体中是否存在 MDR 或中间环丙沙星敏感性,以确定入院时与严重伤寒相关的独立因素。
严重伤寒的患病率为 15.5%(90/581),包括:胃肠道出血(43;7.4%);肝炎(29;5.0%);脑病(16;2.8%);心肌炎(12;2.1%);肠穿孔(6;1.0%);血流动力学休克(5;0.9%)和死亡(3;0.5%)。随着年龄的增长、疾病持续时间的延长以及感染对环丙沙星中介敏感性的生物体,严重疾病更为常见。值得注意的是,MDR 表型与严重疾病无关。严重疾病与感染对环丙沙星中介敏感性的生物体独立相关(AOR 1.90;95%CI 1.18-3.07;p=0.009)和男性(AOR 1.61(1.00-2.57;p=0.035)。
在这群因伤寒住院的患者中,感染对环丙沙星中介敏感性的生物体与疾病严重程度独立相关。在此期间,许多患者在入院前接受了氟喹诺酮类药物治疗。在感染对环丙沙星中介敏感性的伤寒血清 Typhi 患者中,应谨慎使用环丙沙星和氧氟沙星。