Wen Chi Pang, Matsushita Kunihiro, Coresh Josef, Iseki Kunitoshi, Islam Muhammad, Katz Ronit, McClellan William, Peralta Carmen A, Wang HaiYan, de Zeeuw Dick, Astor Brad C, Gansevoort Ron T, Levey Andrew S, Levin Adeera
1] Institute of Population Science, National Health Research Institutes, Zhunan, Taiwan [2] China Medical University Hospital, Taichung, Taiwan.
Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, USA.
Kidney Int. 2014 Oct;86(4):819-27. doi: 10.1038/ki.2013.553. Epub 2014 Feb 12.
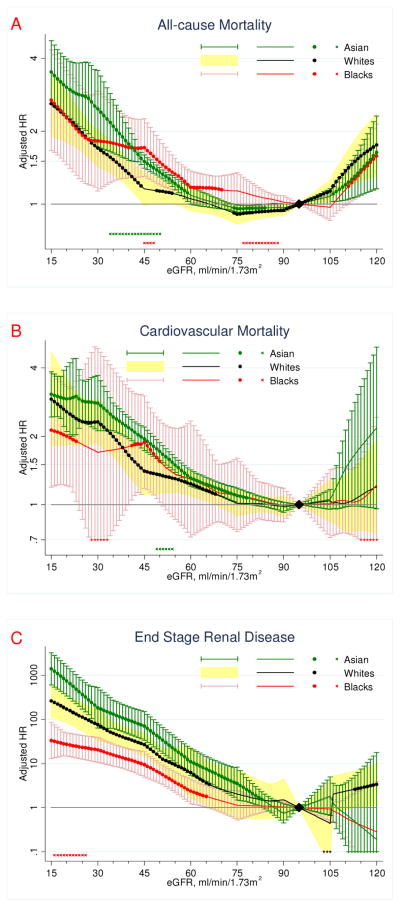
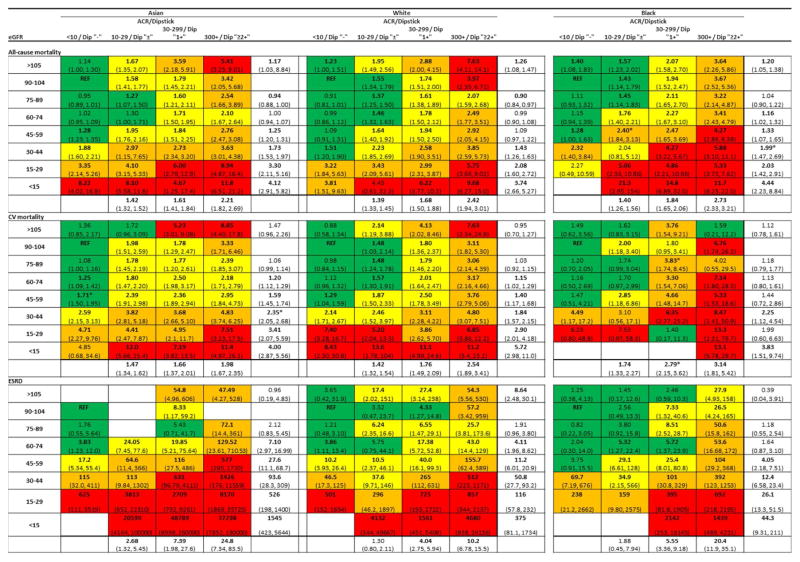
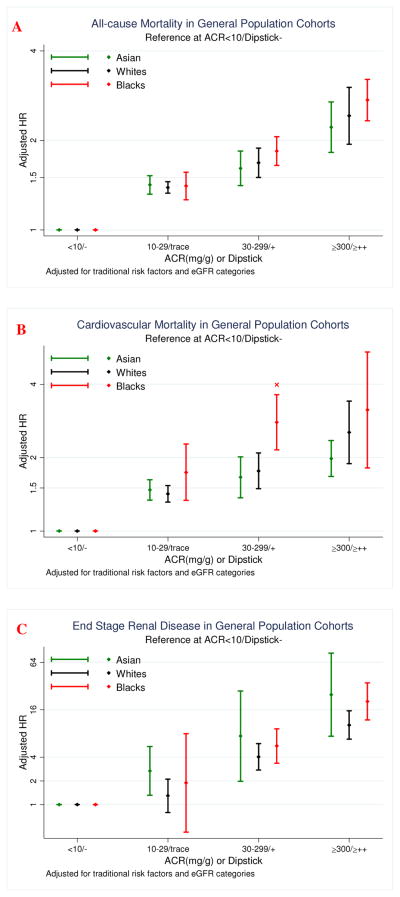
Some suggest race-specific cutpoints for kidney measures to define and stage chronic kidney disease (CKD), but evidence for race-specific clinical impact is limited. To address this issue, we compared hazard ratios of estimated glomerular filtration rates (eGFR) and albuminuria across races using meta-regression in 1.1 million adults (75% Asians, 21% Whites, and 4% Blacks) from 45 cohorts. Results came mainly from 25 general population cohorts comprising 0.9 million individuals. The associations of lower eGFR and higher albuminuria with mortality and end-stage renal disease (ESRD) were largely similar across races. For example, in Asians, Whites, and Blacks, the adjusted hazard ratios (95% confidence interval) for eGFR 45-59 versus 90-104 ml/min per 1.73 m(2) were 1.3 (1.2-1.3), 1.1 (1.0-1.2), and 1.3 (1.1-1.7) for all-cause mortality, 1.6 (1.5-1.7), 1.4 (1.2-1.7), and 1.4 (0.7-2.9) for cardiovascular mortality, and 27.6 (11.1-68.7), 11.2 (6.0-20.9), and 4.1 (2.2-7.5) for ESRD, respectively. The corresponding hazard ratios for urine albumin-to-creatinine ratio 30-299 mg/g or dipstick 1+ versus an albumin-to-creatinine ratio under 10 or dipstick negative were 1.6 (1.4-1.8), 1.7 (1.5-1.9), and 1.8 (1.7-2.1) for all-cause mortality, 1.7 (1.4-2.0), 1.8 (1.5-2.1), and 2.8 (2.2-3.6) for cardiovascular mortality, and 7.4 (2.0-27.6), 4.0 (2.8-5.9), and 5.6 (3.4-9.2) for ESRD, respectively. Thus, the relative mortality or ESRD risks of lower eGFR and higher albuminuria were largely similar among three major races, supporting similar clinical approach to CKD definition and staging, across races.
一些人建议针对肾脏指标设定特定种族的切点来定义和分期慢性肾脏病(CKD),但特定种族临床影响的证据有限。为解决这一问题,我们使用Meta回归分析了来自45个队列的110万成年人(75%为亚洲人,21%为白人,4%为黑人),比较了不同种族间估计肾小球滤过率(eGFR)和蛋白尿的风险比。结果主要来自25个包含90万个体的一般人群队列。较低的eGFR和较高的蛋白尿与死亡率及终末期肾病(ESRD)之间的关联在不同种族中大致相似。例如,在亚洲人、白人和黑人中,eGFR为45 - 59对比90 - 104 ml/min per 1.73 m²时,全因死亡率的调整风险比(95%置信区间)分别为1.3(1.2 - 1.3)、1.1(1.0 - 1.2)和1.3(1.1 - 1.7),心血管死亡率分别为1.6(1.5 - 1.7)、1.4(1.2 - 1.7)和1.4(0.7 - 2.9),ESRD分别为27.6(11.1 - 68.7)、11.2(6.0 - 20.9)和4.1(2.2 - 7.5)。尿白蛋白与肌酐比值为30 - 299 mg/g或试纸法检测为1+对比白蛋白与肌酐比值低于10或试纸法检测为阴性时,全因死亡率的相应风险比分别为1.6(1.4 - 1.8)、1.7(1.5 - 1.9)和1.8(1.7 - 2.1),心血管死亡率分别为1.7(1.4 - 2.0)、1.8(1.5 - 2.1)和2.8(2.2 - 3.6),ESRD分别为7.4(2.0 - 27.6)、4.0(2.8 - 5.9)和5.6(3.4 - 9.2)。因此,较低的eGFR和较高的蛋白尿在三个主要种族中的相对死亡风险或ESRD风险大致相似,支持跨种族对CKD进行定义和分期时采用相似的临床方法。