Service d'Endocrinologie et Diabétologie de l'Enfant Service de Pédiatrie générale - Consultation de rhumatologie Service d'Endocrinologie et des Maladies de la Reproduction Service d'ORL et chirurgie cervico-maxillo-facialeHôpital Bicêtre, APHP, 78 rue du Général Leclerc, 94270 Le Kremlin Bicêtre, France Université Paris 11Faculté de Médecine, Hôpital Bicêtre, 70 rue du Général Leclerc, 94270 Le Kremlin-Bicêtre, France Centre de Référence des Maladies Rares du Métabolisme du Calcium et du PhosphoreLe Kremlin-Bicêtre, France Service d'Odontologie-Maladies Rares Hôpital Bretonneau 2 rue Carpeaux75018 Paris, France Université Paris Descartes 12 Rue de l'École de Médecine75006 Paris, France Service Rhumatologie B Hôpital CochinAPHP, 27, rue du Faubourg Saint-Jacques, 75014 Paris, France Centre de Référence des Maladies Rares des Maladies Auto-Inflammatoires Rares de l'EnfantLe Kremlin Bicêtre, France Service d'explorations fonctionnelles rénales Service de Chirurgie infantile orthopédiqueHôpital Necker-Enfants Malades, 149 rue de Sèvres, 75015 Paris, France Association de patients RVRH-XLH20 rue Merlin de Thionville, 92150 Suresnes, France.
Endocr Connect. 2014 Mar 14;3(1):R13-30. doi: 10.1530/EC-13-0103. Print 2014.
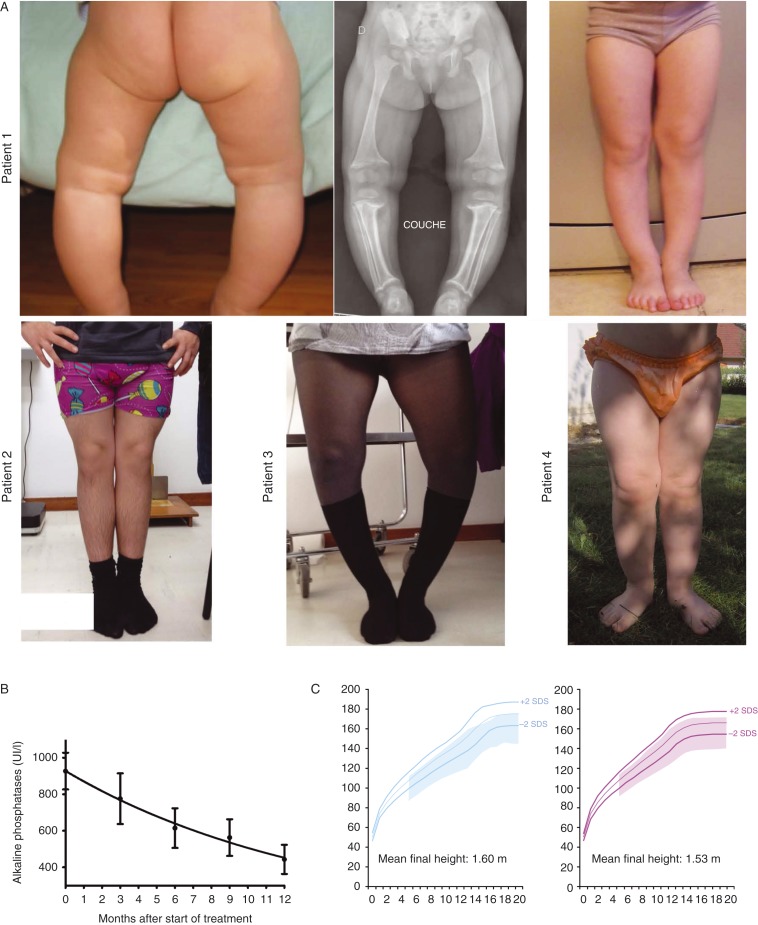
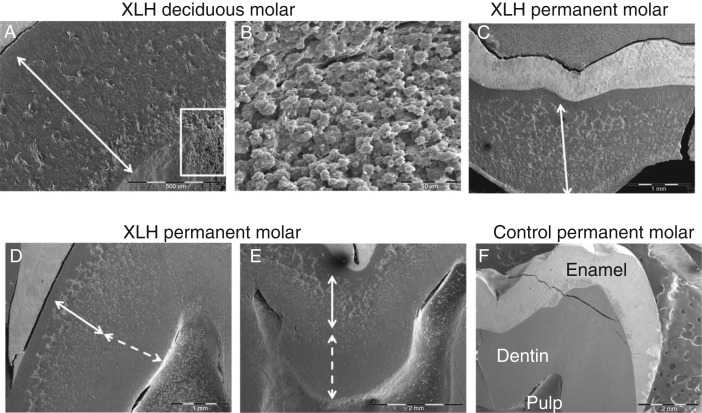
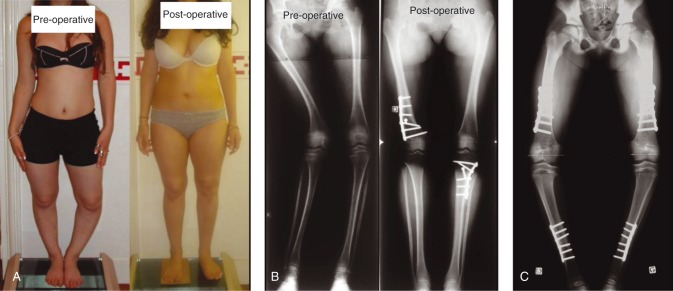
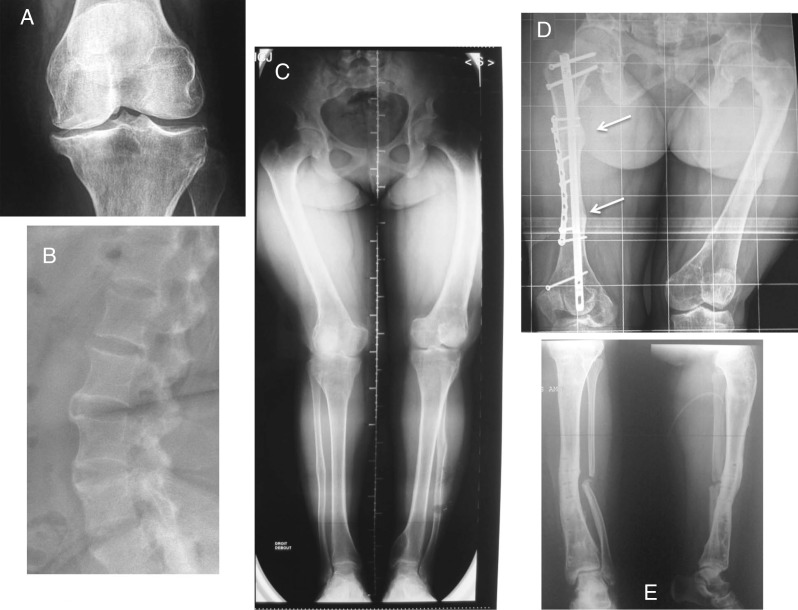
In children, hypophosphatemic rickets (HR) is revealed by delayed walking, waddling gait, leg bowing, enlarged cartilages, bone pain, craniostenosis, spontaneous dental abscesses, and growth failure. If undiagnosed during childhood, patients with hypophosphatemia present with bone and/or joint pain, fractures, mineralization defects such as osteomalacia, entesopathy, severe dental anomalies, hearing loss, and fatigue. Healing rickets is the initial endpoint of treatment in children. Therapy aims at counteracting consequences of FGF23 excess, i.e. oral phosphorus supplementation with multiple daily intakes to compensate for renal phosphate wasting and active vitamin D analogs (alfacalcidol or calcitriol) to counter the 1,25-diOH-vitamin D deficiency. Corrective surgeries for residual leg bowing at the end of growth are occasionally performed. In absence of consensus regarding indications of the treatment in adults, it is generally accepted that medical treatment should be reinitiated (or maintained) in symptomatic patients to reduce pain, which may be due to bone microfractures and/or osteomalacia. In addition to the conventional treatment, optimal care of symptomatic patients requires pharmacological and non-pharmacological management of pain and joint stiffness, through appropriated rehabilitation. Much attention should be given to the dental and periodontal manifestations of HR. Besides vitamin D analogs and phosphate supplements that improve tooth mineralization, rigorous oral hygiene, active endodontic treatment of root abscesses and preventive protection of teeth surfaces are recommended. Current outcomes of this therapy are still not optimal, and therapies targeting the pathophysiology of the disease, i.e. FGF23 excess, are desirable. In this review, medical, dental, surgical, and contributions of various expertises to the treatment of HR are described, with an effort to highlight the importance of coordinated care.
在儿童中,低磷血症性佝偻病(HR)表现为行走延迟、鸭步、下肢弯曲、软骨增大、骨痛、颅缝早闭、自发性牙脓肿和生长发育迟缓。如果在儿童期未被诊断出,低磷血症患者会出现骨骼和/或关节疼痛、骨折、骨软化症等矿化缺陷、肌腱病、严重的牙齿异常、听力损失和疲劳。佝偻病的愈合是儿童治疗的初始终点。治疗旨在对抗 FGF23 过多的后果,即通过多次每日摄入口服补充磷以补偿肾脏磷的丢失,并使用活性维生素 D 类似物(阿尔法骨化醇或骨化三醇)来对抗 1,25-二羟维生素 D 缺乏症。在生长结束时偶尔会对残余下肢弯曲进行矫正手术。由于成人治疗适应症缺乏共识,一般认为应重新开始(或维持)对有症状的患者进行药物治疗,以减轻疼痛,疼痛可能是由于骨微骨折和/或骨软化症引起的。除了常规治疗外,对有症状的患者进行最佳护理还需要通过适当的康复来进行药物和非药物治疗疼痛和关节僵硬。应特别注意 HR 的牙齿和牙周表现。除了改善牙齿矿化的维生素 D 类似物和磷酸盐补充剂外,还建议进行严格的口腔卫生、根尖脓肿的主动根管治疗以及牙齿表面的预防性保护。目前这种治疗的效果仍不理想,针对疾病病理生理学的治疗方法,即 FGF23 过多,是理想的治疗方法。在这篇综述中,描述了 HR 的医学、牙科、手术以及各种专业知识对治疗的贡献,努力强调协调护理的重要性。