Noll Dariusz, Kruk Mariusz, Pręgowski Jerzy, Kaczmarska Edyta, Kryczka Karolina, Pracoń Radosław, Skwarek Mirosław, Dzielińska Zofia, Petryka Joanna, Spiewak Mateusz, Lubiszewska Barbara, Norwa-Otto Bożena, Opolski Maksymilian, Witkowski Adam, Demkow Marcin, Rużyłło Witold, Kępka Cezary
Institute of Cardiology, Warsaw, Poland.
Coronary Disease and Structural Heart Diseases Department, Institute of Cardiology, Warsaw, Poland.
Postepy Kardiol Interwencyjnej. 2013;9(1):1-8. doi: 10.5114/pwki.2013.34022. Epub 2013 Mar 21.
Computed tomography coronary angiography (CTCA) is a diagnostic method used for exclusion of coronary artery disease. However, lower accuracy of CTCA in assessment of calcified lesions is a significant factor impeding applicability of CTCA for assessment of coronary atherosclerosis.
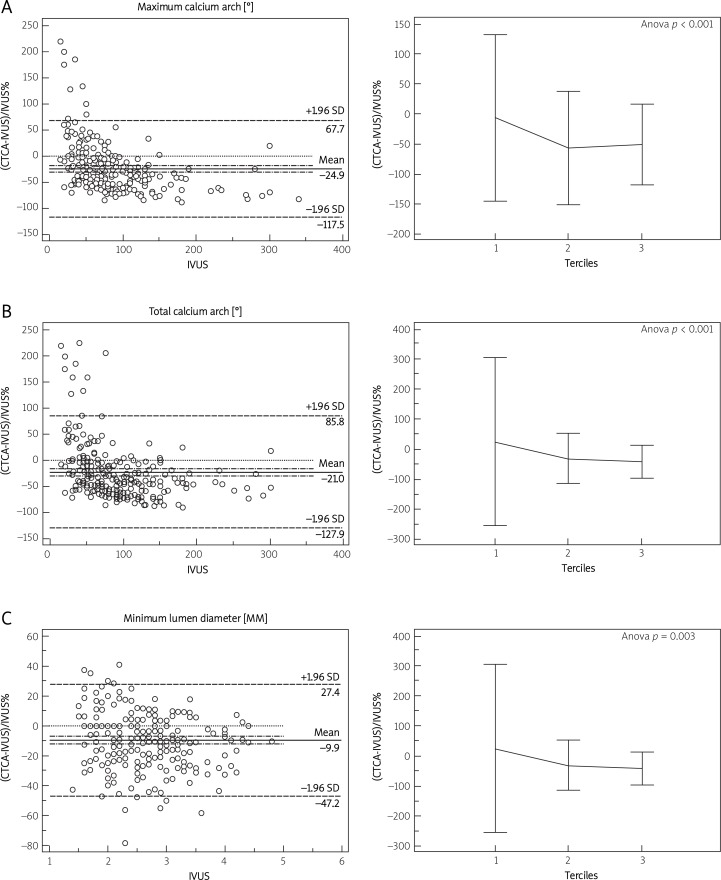
To provide insight into lumen and calcium characteristics assessed with CTCA, we compared these parameters to the reference of intravascular ultrasound (IVUS).
Two hundred and fifty-two calcified lesions within 97 arteries of 60 patients (19 women, age 63 ±10 years) underwent assessment with both 2 × 64 slice CT (Somatom Definition, Siemens) and IVUS (s5, Volcano Corp.). Coronary lumen and calcium dimensions within calcified lesions were assessed with CTCA and compared to the reference measurements made with IVUS.
On average CTCA underestimated mean lumen diameter (2.8 ±0.7 mm vs. 2.9 ±0.8 mm for IVUS), lumen area (6.4 ±3.4 mm(2) vs. 7.0 ±3.7 mm(2) for IVUS, p < 0.001) and total calcium arc (52 ±35° vs. 83 ±54°). However, analysis of tertiles of the examined parameters revealed that the mean lumen diameter, lumen area and calcium arc did not significantly differ between CTCA and IVUS within the smallest lumens (1(st) tertile of mean lumen diameter at 2.1 mm, and 1(st) tertile of lumen area at 3.7 mm(2)) and lowest calcium arc (mean of 40°).
Although, on average, CTCA underestimates lumen diameter and area as well as calcium arc within calcified lesions, the differences are not significant within the smallest vessels and calcium arcs. The low diagnostic accuracy of CTCA within calcified lesions may be attributed to high variance and not to systematic error of measurements.
计算机断层扫描冠状动脉造影(CTCA)是一种用于排除冠状动脉疾病的诊断方法。然而,CTCA在评估钙化病变方面的准确性较低,这是阻碍其用于评估冠状动脉粥样硬化的一个重要因素。
为了深入了解通过CTCA评估的管腔和钙化特征,我们将这些参数与血管内超声(IVUS)的参考值进行了比较。
对60例患者(19名女性,年龄63±10岁)的97条动脉中的252个钙化病变进行了评估,同时使用了2×64层CT(Somatom Definition,西门子)和IVUS(s5,Volcano公司)。通过CTCA评估钙化病变内的冠状动脉管腔和钙化尺寸,并与IVUS的参考测量值进行比较。
平均而言,CTCA低估了平均管腔直径(CTCA为2.8±0.7mm,IVUS为2.9±0.8mm)、管腔面积(CTCA为6.4±3.4mm²,IVUS为7.0±3.7mm²,p<0.001)和总钙化弧(CTCA为52±35°,IVUS为83±54°)。然而,对所检查参数的三分位数分析显示,在最小管腔(平均管腔直径的第1三分位数为2.1mm,管腔面积的第1三分位数为3.7mm²)和最低钙化弧(平均40°)内,CTCA和IVUS之间的平均管腔直径、管腔面积和钙化弧没有显著差异。
虽然平均而言,CTCA低估了钙化病变内的管腔直径、面积以及钙化弧,但在最小血管和钙化弧内差异并不显著。CTCA在钙化病变中的低诊断准确性可能归因于测量的高变异性而非系统误差。