Miltz Ada, Price Huw, Shahmanesh Maryam, Copas Andrew, Gilson Richard
Centre for Sexual Health and HIV Research, Research Department of Infection and Population Health, Mortimer Market Centre, University College London, London, United Kingdom.
PLoS One. 2014 Mar 3;9(3):e90348. doi: 10.1371/journal.pone.0090348. eCollection 2014.
It is unclear whether L1-VLP-based human papillomavirus (HPV) vaccines are efficacious in reducing the likelihood of anogenital pre-cancer in women with evidence of prior vaccine-type HPV exposure. This study aims to determine whether the combined results of the vaccine trials published to date provide evidence of efficacy compared with control (hepatitis A vaccine/placebo).
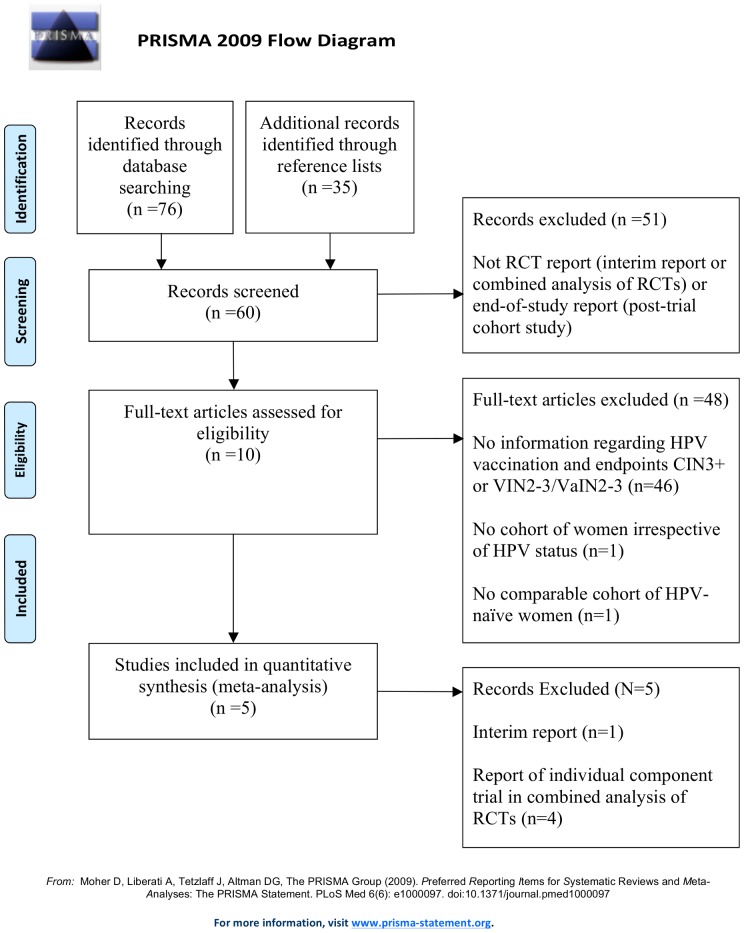
A systematic review and meta-analysis was conducted. Randomized-controlled trials (RCTs) were identified from MEDLINE, Embase, Web of Science, PubMed, Cochrane Central Register of Controlled Trials and references of identified studies. The bivalent vaccine containing HPV-16 and 18 VLPs from GlaxoSmithKline Biologicals (Rixenstart, Belgium), the quadrivalent vaccine containing HPV-6, 11, 16, and 18 VLPs from Merck & Co., Inc., (Whitehouse Station, NJ USA), and the HPV-16 monovalent vaccine from Merck Research Laboratories (West Point, PA USA) were evaluated.
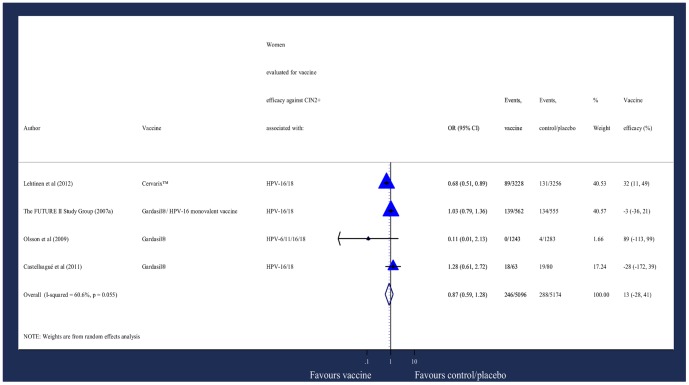
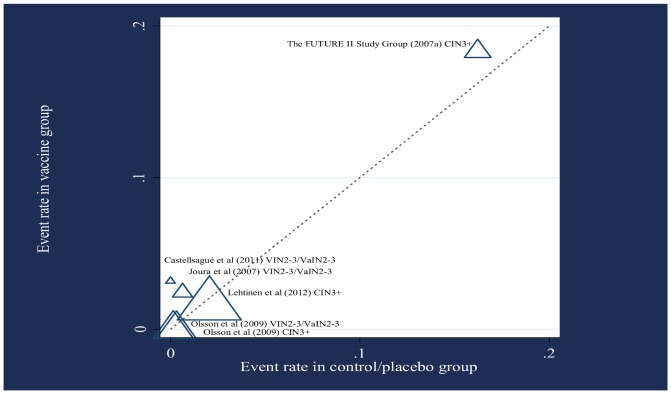
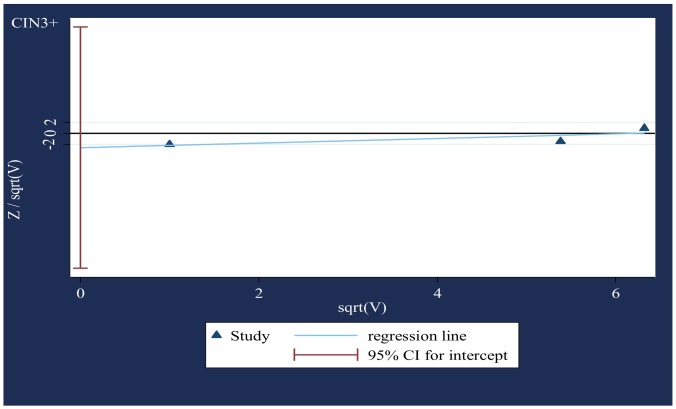
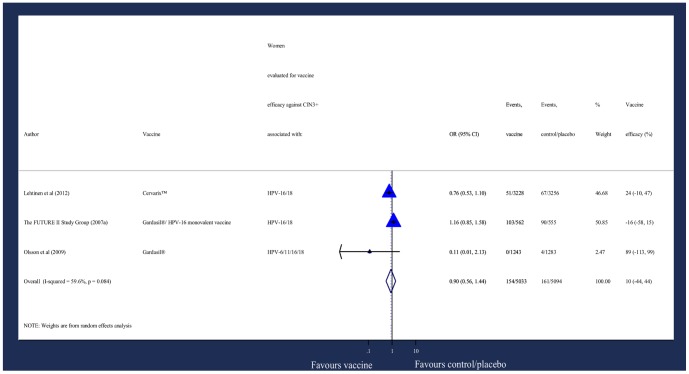
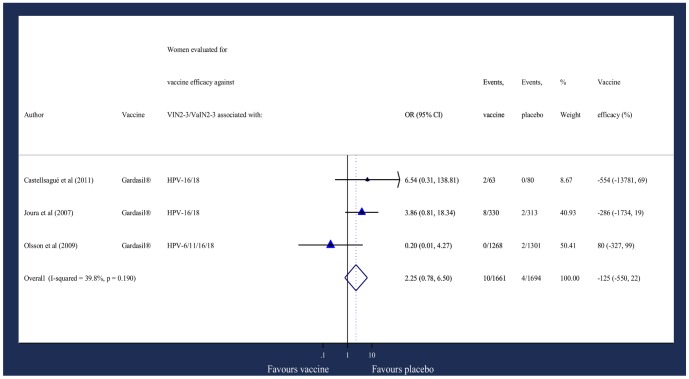
Three RCT reports and two post-trial cohort studies were eligible, comprising data from 13,482 women who were included in the vaccine studies but had evidence of HPV infection at study entry. Data on efficacy was synthesized using the Mantel-Haenszel weighted fixed-effect approach, or where there was heterogeneity between studies, the DerSimonian and Laird weighted random-effect approach. The mean odds ratio (OR) and 95% confidence interval (CI) for the association between Cervarix, Gardasil and HPV-16 monovalent vaccine and HPV-associated cervical intraepithelial neoplasia grade 3 or worse was 0·90 (95% CI: 0·56, 1·44). For the association between Gardasil and HPV-associated vulval/vaginal intraepithelial neoplasia grades 2-3, the overall OR and 95% CI was 2.25 (95% CI: 0·78, 6.50). Sample size and follow-up were limited.
There was no evidence that HPV vaccines are effective in preventing vaccine-type HPV associated pre-cancer in women with evidence of prior HPV exposure. Small effects of vaccination however cannot be excluded and a longer-term benefit in preventing re-infection remains possible.
基于L1病毒样颗粒(VLP)的人乳头瘤病毒(HPV)疫苗对于有证据表明既往暴露于疫苗型HPV的女性,在降低肛门生殖器癌前病变可能性方面是否有效尚不清楚。本研究旨在确定与对照(甲型肝炎疫苗/安慰剂)相比,迄今已发表的疫苗试验的综合结果是否能提供有效性证据。
进行了一项系统综述和荟萃分析。从MEDLINE、Embase、科学网、PubMed、Cochrane对照试验中央注册库以及已识别研究的参考文献中识别随机对照试验(RCT)。对葛兰素史克生物制品公司(比利时里克森斯塔特)生产的含HPV-16和18 VLP的二价疫苗、默克公司(美国新泽西州怀特豪斯站)生产的含HPV-6、11、16和18 VLP的四价疫苗以及默克研究实验室(美国宾夕法尼亚州西点)生产的HPV-16单价疫苗进行了评估。
三项RCT报告和两项试验后队列研究符合条件,包括来自13482名女性的数据,这些女性被纳入疫苗研究,但在研究开始时有HPV感染证据。使用Mantel-Haenszel加权固定效应方法综合疗效数据,或者在研究之间存在异质性时,使用DerSimonian和Laird加权随机效应方法。Cervarix、Gardasil和HPV-16单价疫苗与HPV相关的宫颈上皮内瘤变3级或更严重病变之间关联的平均比值比(OR)和95%置信区间(CI)为0.90(95%CI:0.56,1.44)。对于Gardasil与HPV相关的外阴/阴道上皮内瘤变2-3级之间的关联,总体OR和95%CI为2.25(95%CI:0.78,6.50)。样本量和随访有限。
没有证据表明HPV疫苗对有既往HPV暴露证据的女性预防疫苗型HPV相关癌前病变有效。然而,不能排除疫苗接种的微小效果,并且在预防再次感染方面仍有可能有长期益处。