Valenza Franco, Rosso Lorenzo, Coppola Silvia, Froio Sara, Palleschi Alessandro, Tosi Davide, Mendogni Paolo, Salice Valentina, Ruggeri Giulia M, Fumagalli Jacopo, Villa Alessandro, Nosotti Mario, Santambrogio Luigi, Gattinoni Luciano
Dipartimento di Anestesia Rianimazione (Intensiva e Subintensiva) e Terapia del dolore, Fondazione IRCCS Ca' Granda-Ospedale Maggiore Policlinico, Milano, Italy; Dipartimento di Fisiopatologica Medico-Chirurgica e dei Trapianti, Università degli Studi di Milano, Milano, Italy.
Transpl Int. 2014 Jun;27(6):553-61. doi: 10.1111/tri.12295. Epub 2014 Apr 4.
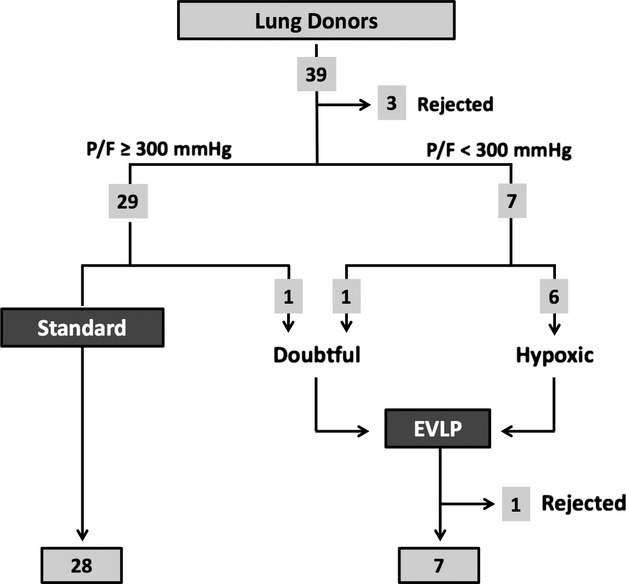
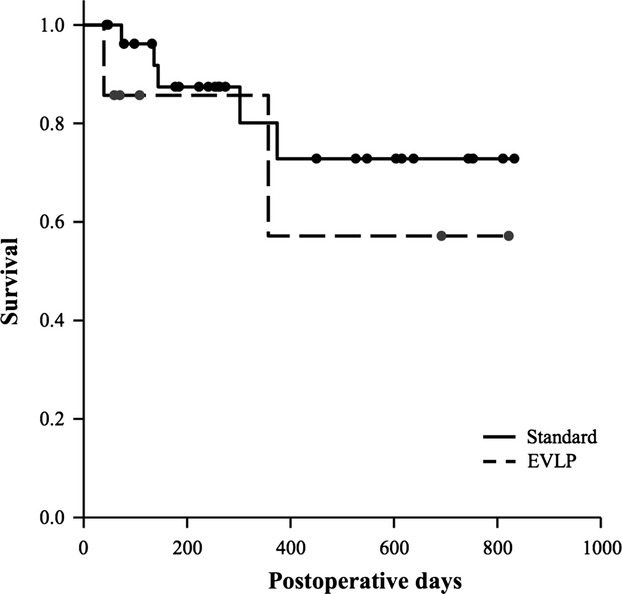
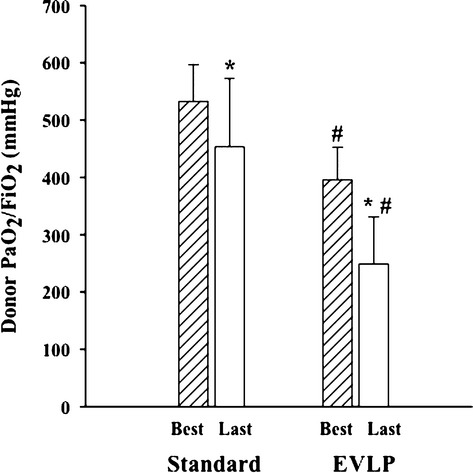
This paper describes the initial clinical experience of ex vivo lung perfusion (EVLP) at the Fondazione Ca' Granda in Milan between January 2011 and May 2013. EVLP was considered if donor PaO2 /FiO2 was below 300 mmHg or if lung function was doubtful. Donors with massive lung contusion, aspiration, purulent secretions, pneumonia, or sepsis were excluded. EVLP was run with a low-flow, open atrium and low hematocrit technique. Thirty-five lung transplants from brain death donors were performed, seven of which after EVLP. EVLP donors were older (54 ± 9 years vs. 40 ± 15 years, EVLP versus Standard, P < 0.05), had lower PaO2 /FiO2 (264 ± 78 mmHg vs. 453 ± 119 mmHg, P < 0.05), and more chest X-ray abnormalities (P < 0.05). EVLP recipients were more often admitted to intensive care unit as urgent cases (57% vs. 18%, P = 0.05); lung allocation score at transplantation was higher (79 [40-84] vs. 39 [36-46], P < 0.05). After transplantation, primary graft dysfunction (PGD72 grade 3, 32% vs. 28%, EVLP versus Standard, P = 1), mortality at 30 days (0% vs. 0%, P = 1), and overall survival (71% vs. 86%, EVLP versus Standard P = 0.27) were not different between groups. EVLP enabled a 20% increase in available donor organs and resulted in successful transplants with lungs that would have otherwise been rejected (ClinicalTrials.gov number: NCT01967953).
本文描述了2011年1月至2013年5月期间米兰圣心医院进行体外肺灌注(EVLP)的初步临床经验。如果供体动脉血氧分压/吸入氧分数值(PaO2/FiO2)低于300mmHg或肺功能存疑,则考虑进行EVLP。排除有严重肺挫伤、误吸、脓性分泌物、肺炎或脓毒症的供体。EVLP采用低流量、开放心房和低血细胞比容技术进行。共进行了35例脑死亡供体的肺移植,其中7例在EVLP后进行。EVLP供体年龄更大(54±9岁 vs. 40±15岁,EVLP组与标准组,P<0.05),PaO2/FiO2更低(264±78mmHg vs. 453±119mmHg,P<0.05),胸部X线异常更多(P<0.05)。EVLP受者作为紧急病例更常入住重症监护病房(57% vs. 18%,P = 0.05);移植时的肺分配评分更高(79[40 - 84] vs. 39[36 - 46],P<0.05)。移植后,原发性移植物功能障碍(PGD72 3级,32% vs. 28%,EVLP组与标准组,P = 1)、30天死亡率(0% vs. 0%,P = 1)和总体生存率(71% vs. 86%,EVLP组与标准组,P = 0.27)在两组之间无差异。EVLP使可用供体器官增加了20%,并成功移植了原本会被拒绝的肺(临床试验注册号:NCT01967953)。