Hospices Civils de Lyon, Centre Hospitalier Lyon-Sud, Service de Chirurgie Viscérale et Endocrinienne, Pierre-Bénite Cedex 69495, France.
BMC Cancer. 2014 Mar 14;14:183. doi: 10.1186/1471-2407-14-183.
In Europe, gastric cancer remains diagnosed at advanced stage (serosal and/or lymph node involvement). Despite curative management combining perioperative systemic chemotherapy and gastrectomy with D1-D2 lymph node dissection, 5-year survival rates of T3 and/or N + patients remain under 30%. More than 50% of recurrences are peritoneal and/or locoregional. The use of adjuvant hyperthermic intraperitoneal chemotherapy that eliminates free cancer cells that can be released into peritoneal cavity during the gastrectomy and prevents peritoneal carcinomatosis recurrences, was extensively evaluated by several randomized trials conducted in Asia. Two meta-analysis reported that adjuvant hyperthermic intraperitoneal chemotherapy significantly reduces the peritoneal recurrences and significantly improves the overall survival. As it was previously done for the evaluation of the extension of lymph node dissection, it seems very important to validate on European or caucasian patients the results observed in trials performed in Asia.
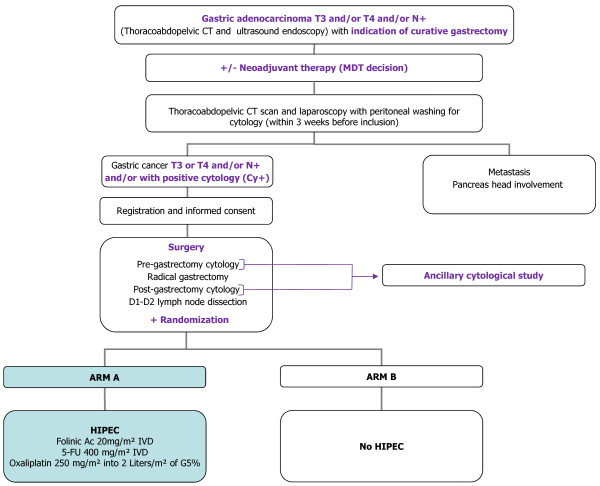
METHODS/DESIGN: GASTRICHIP is a prospective, open, randomized multicenter phase III clinical study with two arms that aims to evaluate the effects of hyperthermic intraperitoneal chemotherapy with oxaliplatin on patients with gastric cancer involving the serosa and/or lymph node involvement and/or with positive cytology at peritoneal washing, treated with perioperative systemic chemotherapy and D1-D2 curative gastrectomy. Peroperatively, at the end of curative surgery, patients will be randomized after preoperatively written consent has been given for participation. Primary endpoint will be overall survival from the date of surgery to the date of death or to the end of follow-up (5 years). Secondary endpoint will be 3- and 5-year recurrence-free survival, site of recurrence, morbidity, and quality of life. An ancillary study will compare the incidence of positive peritoneal cytology pre- and post-gastrectomy in two arms of the study, and assess its impact on 5-year survival. The number of patients to be randomized was calculated to be 306.
EudraCT number: 2012-005748-12, ClinicalTrials.gov identifier: NCT01882933.
在欧洲,胃癌仍然被诊断为晚期(累及浆膜和/或淋巴结)。尽管采用了包括围手术期全身化疗和 D1-D2 淋巴结清扫术在内的根治性治疗,但 T3 和/或 N+患者的 5 年生存率仍低于 30%。超过 50%的复发是腹膜内和/或局部区域的。多项亚洲开展的随机试验广泛评估了使用辅助腹腔内热化疗,该方法可以清除胃癌手术过程中可能释放到腹腔内的游离癌细胞,从而预防腹膜癌复发。两项荟萃分析报告称,辅助腹腔内热化疗可显著降低腹膜复发率,并显著提高总生存率。正如之前对淋巴结清扫范围的评估一样,在欧洲或白种人群中验证亚洲试验中观察到的结果似乎非常重要。
方法/设计:GASTRICHIP 是一项前瞻性、开放性、随机、多中心 III 期临床研究,分为两组,旨在评估奥沙利铂腹腔内热化疗对浆膜和/或淋巴结受累和/或腹腔冲洗阳性细胞学的胃癌患者的疗效,这些患者接受了围手术期全身化疗和根治性 D1-D2 胃切除术。在手术结束时,经过术前书面同意参与研究后,患者将被随机分组。主要终点是从手术日期到死亡日期或随访结束日期(5 年)的总生存率。次要终点是 3 年和 5 年无复发生存率、复发部位、发病率和生活质量。一项辅助研究将比较研究中两组术前和术后腹腔细胞学阳性的发生率,并评估其对 5 年生存率的影响。随机分组的患者数量计算为 306 例。
EudraCT 编号:2012-005748-12,ClinicalTrials.gov 标识符:NCT01882933。