Department of Management Science and Engineering, Stanford University, Stanford, CA, USA.
BMC Med. 2014 Mar 17;12:46. doi: 10.1186/1741-7015-12-46.
Antiretroviral therapy (ART) and oral pre-exposure prophylaxis (PrEP) are effective in reducing HIV transmission in heterosexual adults. The epidemiologic impact and cost-effectiveness of combined prevention approaches in resource-limited settings remain unclear.
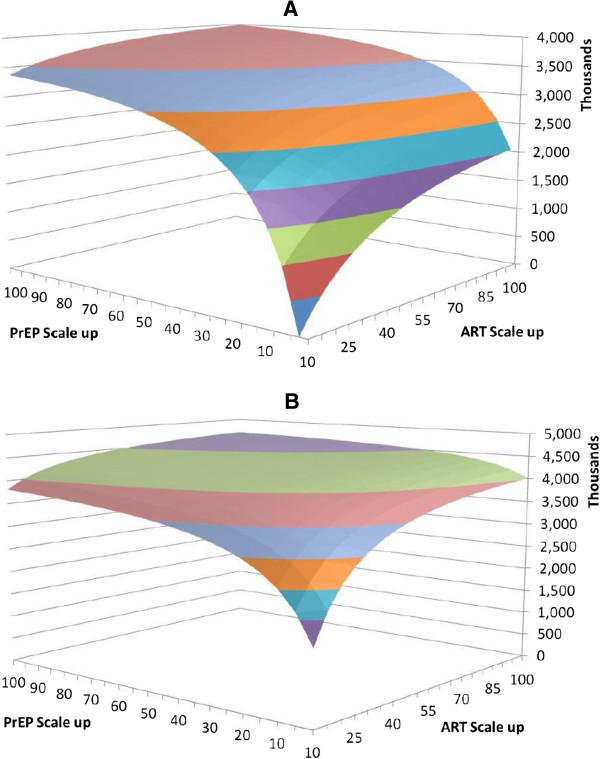
We develop a dynamic mathematical model of the HIV epidemic in South Africa's adult population. We assume ART reduces HIV transmission by 95% and PrEP by 60%. We model two ART strategies: scaling up access for those with CD4 counts ≤ 350 cells/μL (Guidelines) and for all identified HIV-infected individuals (Universal). PrEP strategies include use in the general population (General) and in high-risk individuals (Focused). We consider strategies where ART, PrEP, or both are scaled up to 100% of remaining eligible individuals yearly. We measure infections averted, quality-adjusted life-years (QALYs) gained and incremental cost-effectiveness ratios over 20 years.
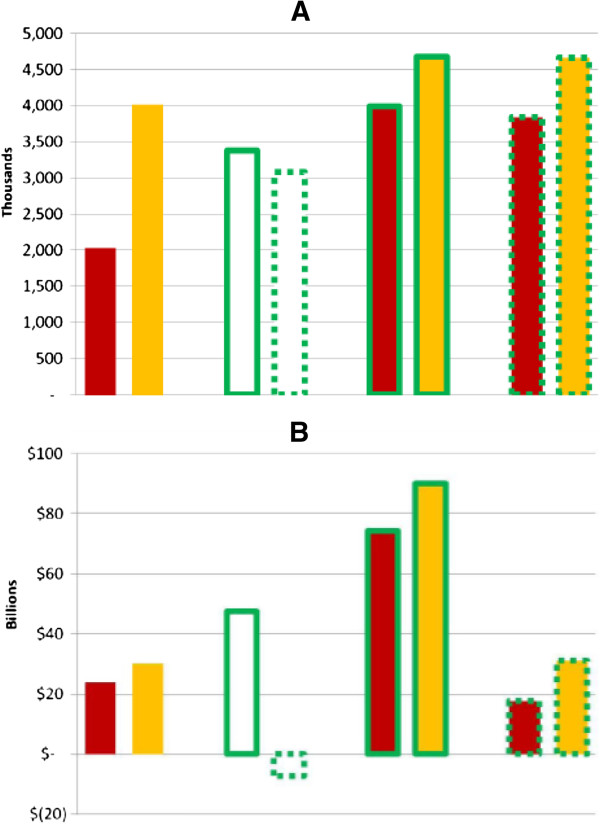
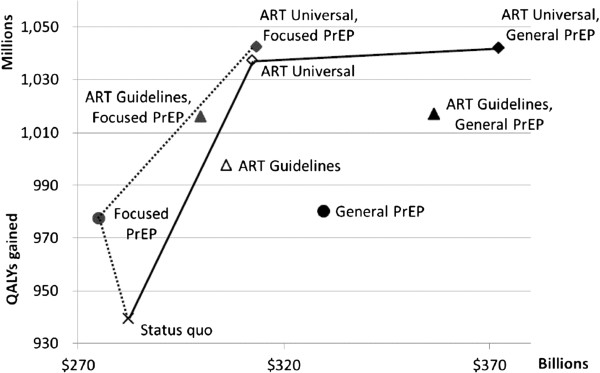
Scaling up ART to 50% of eligible individuals averts 1,513,000 infections over 20 years (Guidelines) and 3,591,000 infections (Universal). Universal ART is the most cost-effective strategy at any scale ($160-$220/QALY versus comparable scale Guidelines ART expansion). General PrEP is costly and provides limited benefits beyond ART scale-up ($7,680/QALY to add 100% PrEP to 50% Universal ART). Cost-effectiveness of General PrEP becomes less favorable when ART is widely given ($12,640/QALY gained when added to 100% Universal ART). If feasible, Focused PrEP is cost saving or highly cost effective versus status quo and when added to ART strategies.
Expanded ART coverage to individuals in early disease stages may be more cost-effective than current guidelines. PrEP can be cost-saving if delivered to individuals at increased risk of infection.
抗逆转录病毒疗法(ART)和口服暴露前预防(PrEP)可有效降低异性恋成年人中的 HIV 传播。在资源有限的环境中,联合预防方法的流行病学影响和成本效益仍不清楚。
我们建立了南非成年人中 HIV 流行的动态数学模型。我们假设 ART 将 HIV 传播减少 95%,PrEP 将 HIV 传播减少 60%。我们构建了两种 ART 策略:扩大 CD4 计数≤350 个细胞/μL(指南)的人群和所有已确定的 HIV 感染者(通用)的 ART 获得途径。PrEP 策略包括在普通人群(一般)和高危人群(重点)中使用。我们考虑每年将 ART、PrEP 或两者都扩大到剩余符合条件的个体的 100%的策略。我们衡量在 20 年内避免的感染、获得的质量调整生命年(QALY)和增量成本效益比。
将 ART 扩大到 50%的符合条件的个体可在 20 年内避免 151.3 万例感染(指南)和 359.1 万例感染(通用)。通用 ART 在任何规模下都是最具成本效益的策略(160-220 美元/QALY,与可比规模的指南 ART 扩展相比)。一般 PrEP 的成本较高,并且在扩大 ART 规模之外提供的益处有限(增加 100%PrEP 至 50%通用 ART 可获得 7680 美元/QALY)。当广泛提供 ART 时,一般 PrEP 的成本效益变得不那么有利(添加到 100%通用 ART 时获得 12640 美元/QALY)。如果可行,与现状相比,重点 PrEP 具有成本效益或极具成本效益,并且可以添加到 ART 策略中。
将 ART 覆盖范围扩大到早期疾病阶段的个体可能比当前指南更具成本效益。如果提供给感染风险增加的个体,PrEP 可以节省成本。