Department of Medical Social Sciences, Northwestern University Feinberg School of Medicine, Chicago, Illinois.
Cancer. 2014 Jun 15;120(12):1871-80. doi: 10.1002/cncr.28660. Epub 2014 Mar 13.
Using phase 3 trial data for sunitinib versus interferon (IFN)-α in treatment-naive patients with metastatic renal cell carcinoma, retrospective analyses characterized sunitinib-associated fatigue and its impact on patient-reported health-related quality of life (HRQoL).
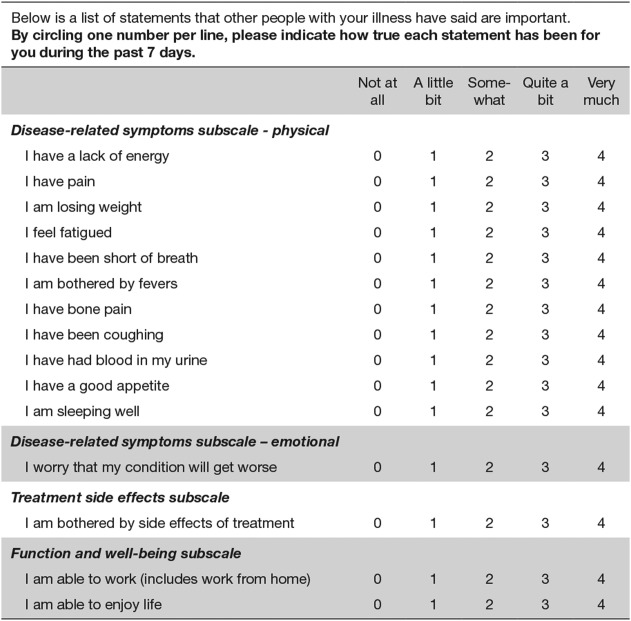
Patients received sunitinib at a dose of 50 mg/day on a schedule of 4 weeks on/2 weeks off (375 patients) or IFN-α at a dose of 9 MU subcutaneously 3 times per week (360 patients). HRQoL was self-assessed using the Functional Assessment of Cancer Therapy-Kidney Symptom Index-15-item (FKSI-15) questionnaire, with fatigue assessed using its Disease-Related Symptoms subscale. Fatigue was also assessed by providers using Common Terminology Criteria for Adverse Events (CTCAE). A repeated-measures model (M1) and random intercept-slope model (M2) characterized sunitinib-associated fatigue over time. Another repeated-measures model examined the relationship between HRQoL scores and CTCAE fatigue grade.
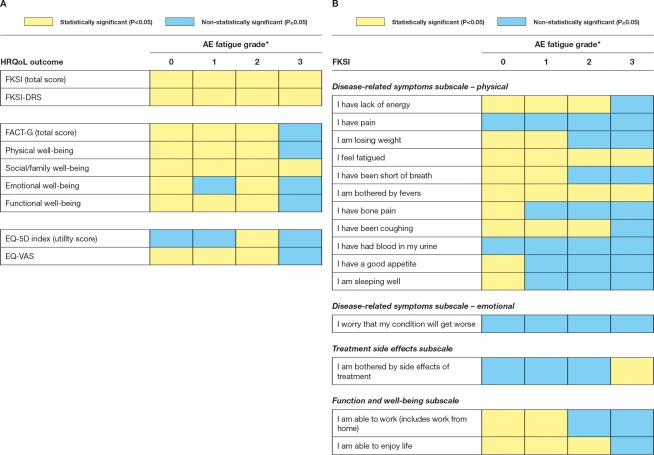
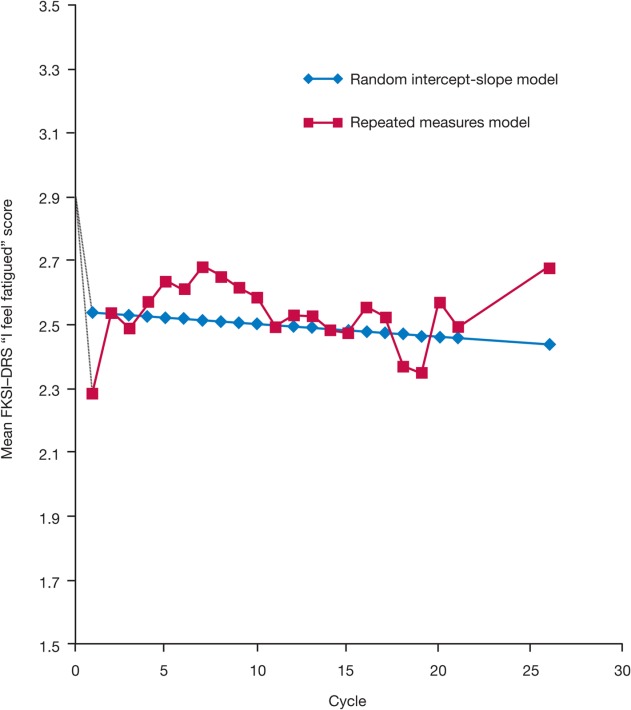
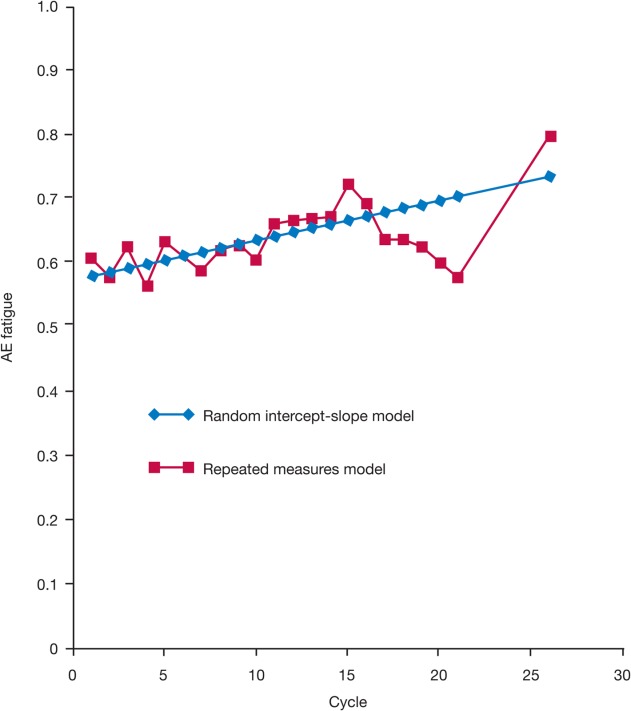
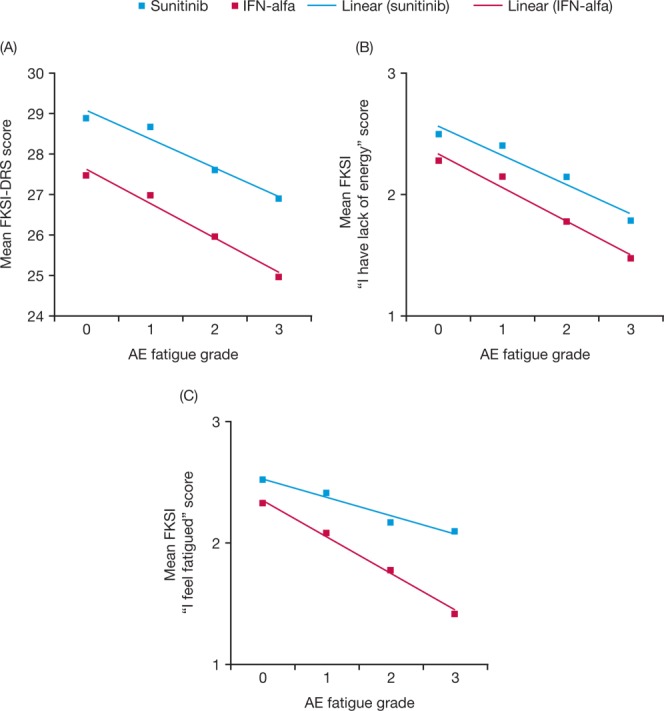
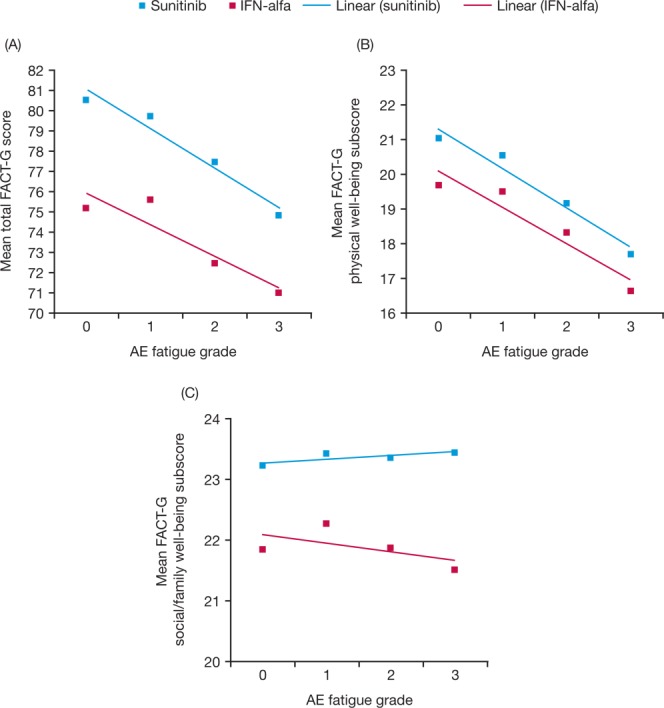
M1 demonstrated that the initial increase in patient-reported fatigue with sunitinib was worst during cycle 1, with mean values numerically better at subsequent cycles; most pairwise comparisons of consecutive CTCAE fatigue cycle means were not found to be statistically significant. M2 demonstrated that the overall trend (slope) for patient-reported and CTCAE fatigue with sunitinib was not statistically different from 0. The relationship between most HRQoL scores and CTCAE fatigue was close to linear regardless of treatment, with lower scores (worse HRQoL) corresponding to higher fatigue grade. The majority of HRQoL scores were better with sunitinib versus IFN-α for the same CTCAE fatigue grade.
Patients reported worse fatigue during the first sunitinib cycle. However, in subsequent consecutive cycles, less fatigue was reported with no statistically significant worsening. CTCAE fatigue assessment may not fully capture patient treatment experience.
利用转移性肾细胞癌初治患者的 3 期试验数据对舒尼替尼与干扰素(IFN)-α进行回顾性分析,以评估舒尼替尼相关乏力及其对患者报告的健康相关生活质量(HRQoL)的影响。
患者接受舒尼替尼 50mg/天治疗,方案为 4 周用药/2 周停药(375 例)或 IFN-α 9MU 皮下每周 3 次(360 例)。采用癌症治疗功能评估-肾脏症状指数 15 项(FKSI-15)问卷自我评估 HRQoL,采用疾病相关症状亚量表评估乏力。采用常见不良事件术语标准(CTCAE)评估乏力也由提供者进行评估。采用重复测量模型(M1)和随机截距斜率模型(M2)描述舒尼替尼相关乏力随时间的变化。另一个重复测量模型检查了 HRQoL 评分与 CTCAE 乏力等级之间的关系。
M1 表明,舒尼替尼引起的患者报告乏力最初在第 1 个周期中增加最严重,随后的周期中均值数值更好;连续 CTCAE 乏力周期均值的大多数两两比较均无统计学意义。M2 表明,舒尼替尼引起的患者报告和 CTCAE 乏力的总体趋势(斜率)与 0 无统计学差异。无论治疗如何,HRQoL 评分与 CTCAE 乏力之间的关系均接近线性,较低的评分(较差的 HRQoL)对应较高的乏力等级。在相同的 CTCAE 乏力等级下,大多数 HRQoL 评分在舒尼替尼治疗时优于 IFN-α。
患者在第 1 个舒尼替尼周期报告更严重的乏力。然而,在随后的连续周期中,报告的乏力程度较轻,无统计学意义的恶化。CTCAE 乏力评估可能无法完全捕捉患者的治疗体验。