Shalhub Sherene, Black James H, Cecchi Alana C, Xu Zhi, Griswold Ben F, Safi Hazim J, Milewicz Dianna M, McDonnell Nazli B
Division of Vascular Surgery, Department of General Surgery, University of Washington, Seattle, Wash.
Division of Vascular Surgery and Endovascular Therapy, Department of Surgery, The Johns Hopkins Hospital, Baltimore, Md.
J Vasc Surg. 2014 Jul;60(1):160-9. doi: 10.1016/j.jvs.2014.01.070. Epub 2014 Mar 18.
The management of arterial pathology in individuals with vascular Ehlers-Danlos syndrome (vEDS) remains a challenge. Here we describe the correlation between COL3A1 gene mutation type and the clinical phenotype in individuals with vEDS.
Individuals with confirmed molecular diagnoses of vEDS were enrolled in a multi-institutional natural history study. Data collected included demographics, clinical and family histories, arterial pathology (aneurysm, dissection, and rupture), operative details, and autopsy reports. Individuals were classified into two cohorts by the type of COL3A1 mutations and their effect on the amount of normal collagen produced: those with mutations that lead to minimal (MIN) production (10%-15%) of normal type III collagen and those with haploinsufficiency (HI) mutations that lead to production of 50% of the normal type III collagen.
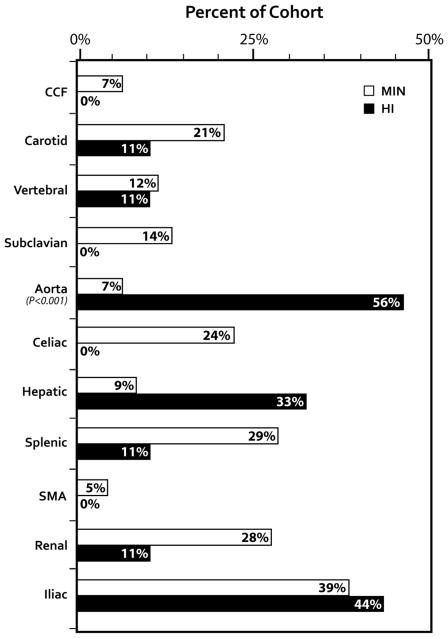
A cohort of 68 individuals (72%) from 56 families had arterial pathology (44% male) with 13% HI. The HI group was older at the time of their first vascular event (mean, 42 [range, 26-58] years vs 33 [range, 8-62] years; P = .016) and had a higher incidence of aortic pathology than the MIN group (56% vs 21%; P = .025). Visceral arterial pathology was seen in 43 arteries in 23 individuals in the MIN group vs only one artery in five individuals in the HI group. Emergency surgical procedures were more likely to be undertaken when vEDS diagnosis was not known (81% vs 41%; P = .005), and 81% of these procedures were open surgical repair compared with 19% endovascular repairs (P = .019). Open and endovascular repairs were equally used in the elective setting. Postoperative complications were highest when the diagnosis of vEDS was not known (62% vs 14%; P < .001) and when procedures were undertaken in an emergency setting (5% vs 55% P < .001). Mortality due to arterial complications was 0% in the HI cohort and 21% in the MIN cohort (P = .132).
Arterial pathology in vEDS individuals is related to the underlying COL3A1 mutation type. The arterial pathology in individuals with HI mutations occurs at later ages with a higher incidence of aortic disease compared with other COL3A1 mutation types. Molecular diagnosis is recommended because diagnosis confirmation, appropriate surveillance, and prophylactic interventions in an elective setting improve surgical outcomes.
血管性埃勒斯-当洛综合征(vEDS)患者的动脉病变管理仍然是一项挑战。在此,我们描述vEDS患者中COL3A1基因突变类型与临床表型之间的相关性。
确诊为vEDS的患者被纳入一项多机构自然史研究。收集的数据包括人口统计学、临床和家族史、动脉病变(动脉瘤、夹层和破裂)、手术细节及尸检报告。根据COL3A1突变类型及其对正常胶原蛋白产生量的影响,将患者分为两个队列:导致正常III型胶原蛋白产生量极少(MIN)(10%-15%)的突变患者和导致产生50%正常III型胶原蛋白的单倍体不足(HI)突变患者。
来自56个家庭的68名患者(72%)有动脉病变(男性占44%),其中13%为HI型。HI组首次发生血管事件时年龄较大(平均42岁[范围26-58岁],而MIN组为33岁[范围8-62岁];P = 0.016),且主动脉病变发生率高于MIN组(56%对21%;P = 0.025)。MIN组23名患者的43条内脏动脉出现病变,而HI组5名患者仅1条动脉出现病变。当vEDS诊断未明确时,更有可能进行急诊手术(81%对41%;P = 0.005),其中81%的手术为开放手术修复,而血管内修复仅占19%(P = 0.019)。在择期手术中,开放手术和血管内修复的使用频率相同。当vEDS诊断未明确时,术后并发症发生率最高(62%对14%;P < 0.001),且在急诊情况下进行手术时并发症发生率也最高(5%对55%,P < 0.001)。HI队列中因动脉并发症导致的死亡率为0%,MIN队列中为21%(P = 0.132)。
vEDS患者的动脉病变与潜在的COL3A1突变类型有关。与其他COL3A1突变类型相比,HI突变患者的动脉病变发生年龄较晚,主动脉疾病发生率较高。建议进行分子诊断,因为确诊、适当监测以及在择期情况下进行预防性干预可改善手术结果。