Liu Yao, Liu Yi, Su Lili, Jiang Shu-juan
Department of Respiratory Medicine, Provincial Hospital Affiliated to Shandong University, Jinan, Shandong, China.
PLoS One. 2014 Mar 21;9(3):e92773. doi: 10.1371/journal.pone.0092773. eCollection 2014.
Primary graft dysfunction (PGD) is the main cause of early morbidity and mortality after lung transplantation. Previous studies have yielded conflicting results for PGD risk factors. Herein, we carried out a systematic review and meta-analysis of published literature to identify recipient-related clinical risk factors associated with PGD development.
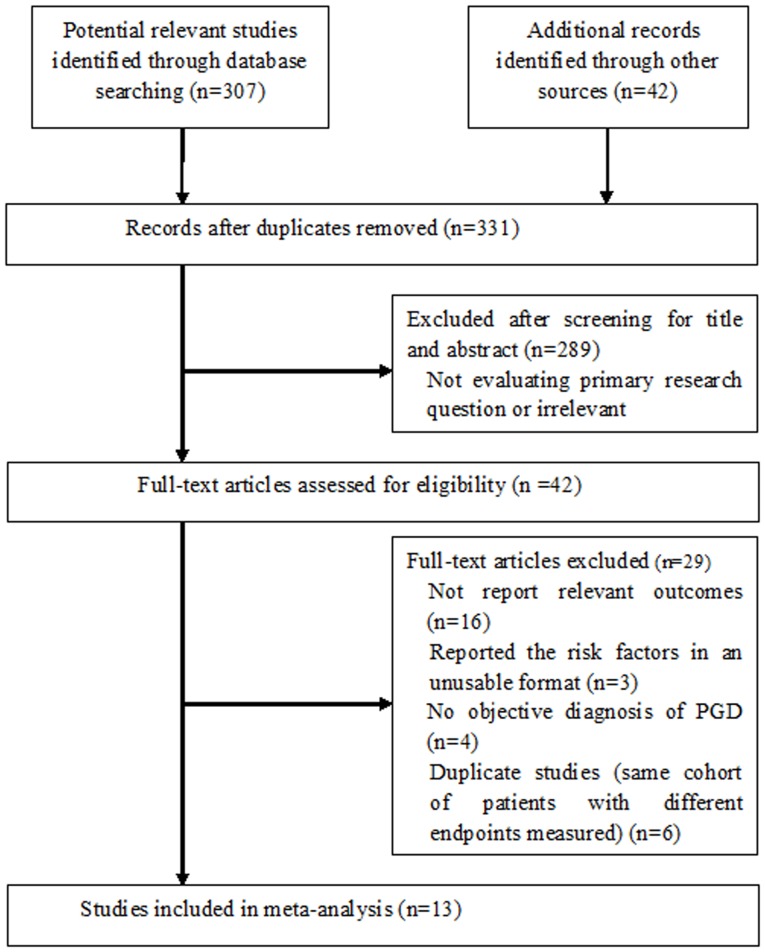
A systematic search of electronic databases (PubMed, Embase, Web of Science, Cochrane CENTRAL, and Scopus) for studies published from 1970 to 2013 was performed. Cohort, case-control, or cross-sectional studies that examined recipient-related risk factors of PGD were included. The odds ratios (ORs) or mean differences (MDs) were calculated using random-effects models.
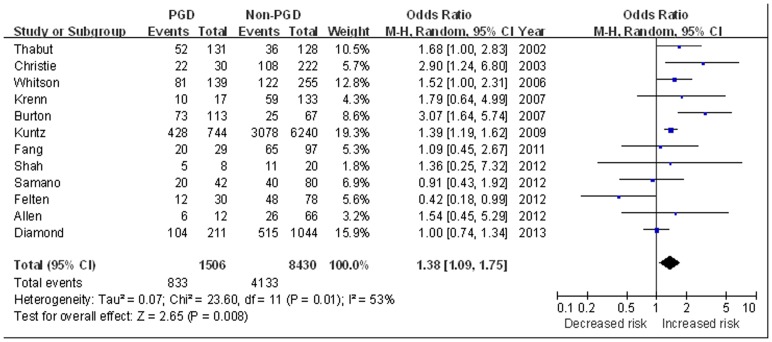
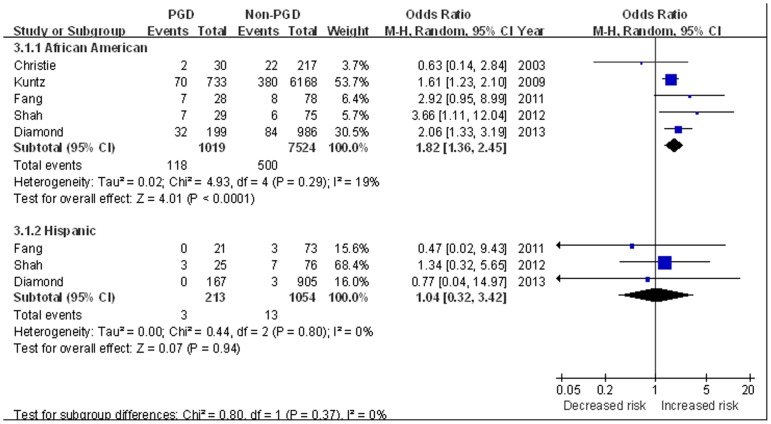
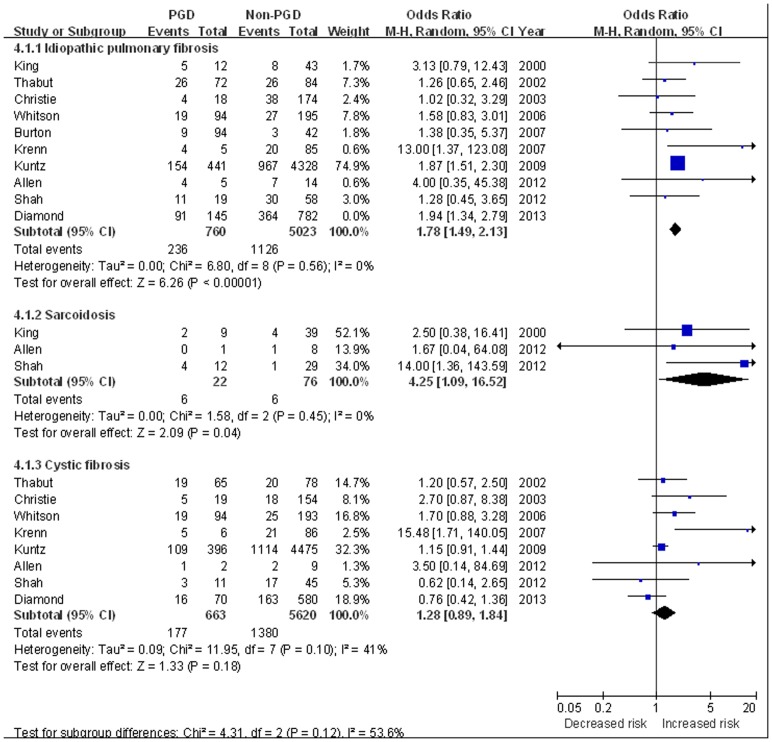
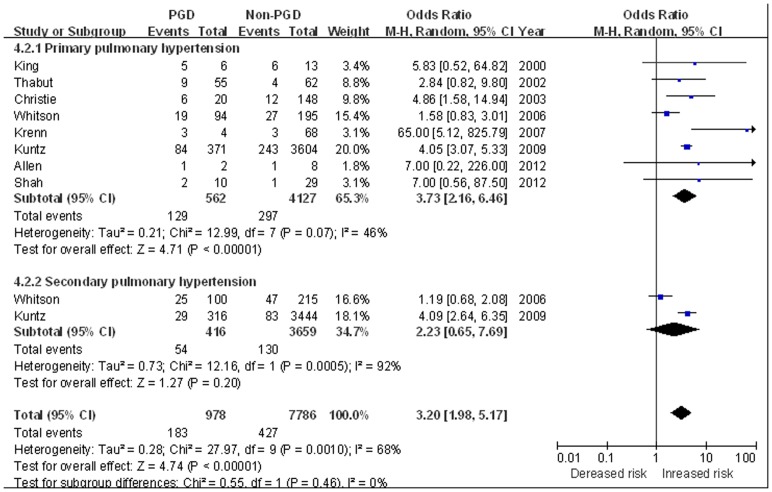
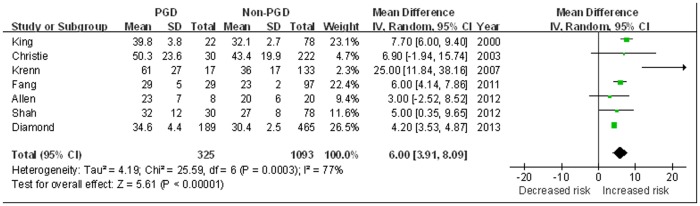
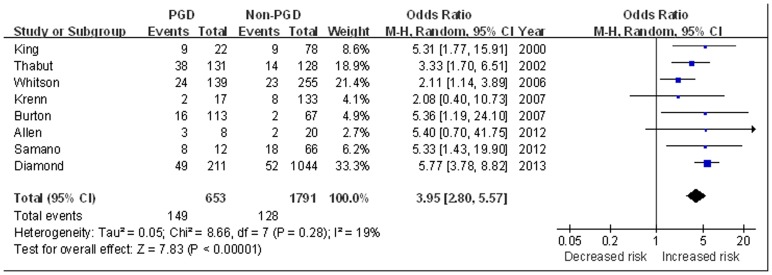
Thirteen studies involving 10042 recipients met final inclusion criteria. From the pooled analyses, female gender (OR 1.38, 95% CI 1.09 to 1.75), African American (OR 1.82, 95%CI 1.36 to 2.45), idiopathic pulmonary fibrosis (IPF) (OR 1.78, 95% CI 1.49 to 2.13), sarcoidosis (OR 4.25, 95% CI 1.09 to 16.52), primary pulmonary hypertension (PPH) (OR 3.73, 95%CI 2.16 to 6.46), elevated BMI (BMI≥25 kg/m2) (OR 1.83, 95% CI 1.26 to 2.64), and use of cardiopulmonary bypass (CPB) (OR 2.29, 95%CI 1.43 to 3.65) were significantly associated with increased risk of PGD. Age, cystic fibrosis, secondary pulmonary hypertension (SPH), intra-operative inhaled nitric oxide (NO), or lung transplant type (single or bilateral) were not significantly associated with PGD development (all P>0.05). Moreover, a nearly 4 fold increased risk of short-term mortality was observed in patients with PGD (OR 3.95, 95% CI 2.80 to 5.57).
Our analysis identified several recipient related risk factors for development of PGD. The identification of higher-risk recipients and further research into the underlying mechanisms may lead to selective therapies aimed at reducing this reperfusion injury.
原发性移植肺功能障碍(PGD)是肺移植术后早期发病和死亡的主要原因。以往关于PGD危险因素的研究结果相互矛盾。在此,我们对已发表的文献进行了系统评价和荟萃分析,以确定与PGD发生相关的受者相关临床危险因素。
对1970年至2013年发表的研究在电子数据库(PubMed、Embase、Web of Science、Cochrane CENTRAL和Scopus)中进行系统检索。纳入了检查PGD受者相关危险因素的队列研究、病例对照研究或横断面研究。使用随机效应模型计算比值比(OR)或平均差(MD)。
13项涉及10042名受者的研究符合最终纳入标准。汇总分析显示,女性(OR 1.38,95%CI 1.09至1.75)、非裔美国人(OR 1.82,95%CI 1.36至2.45)、特发性肺纤维化(IPF)(OR 1.78,95%CI 1.49至2.13)、结节病(OR 4.25,95%CI 1.09至16.52)、原发性肺动脉高压(PPH)(OR 3.73,95%CI 2.16至6.46)、BMI升高(BMI≥25 kg/m2)(OR 1.83,95%CI 1.26至2.64)以及使用体外循环(CPB)(OR 2.29,95%CI 1.43至3.65)与PGD风险增加显著相关。年龄、囊性纤维化、继发性肺动脉高压(SPH)、术中吸入一氧化氮(NO)或肺移植类型(单肺或双肺)与PGD发生无显著相关性(所有P>0.05)。此外,PGD患者短期死亡风险增加近4倍(OR 3.95,95%CI 2.80至5.57)。
我们的分析确定了几个与PGD发生相关的受者相关危险因素。识别高危受者并进一步研究潜在机制可能会导致旨在减少这种再灌注损伤的选择性治疗。