Xiao Ying, Papiez Lech, Paulus Rebecca, Timmerman Robert, Straube William L, Bosch Walter R, Michalski Jeff, Galvin James M
Department of Radiation Oncology, Jefferson Medical College, Philadelphia, PA 19107, USA.
Int J Radiat Oncol Biol Phys. 2009 Mar 15;73(4):1235-42. doi: 10.1016/j.ijrobp.2008.11.019.
Using a retrospective analysis of treatment plans submitted from multiple institutions accruing patients to the Radiation Therapy Oncology Group (RTOG) 0236 non-small-cell stereotactic body radiotherapy protocol, the present study determined the dose prescription and critical structure constraints for future stereotactic body radiotherapy lung protocols that mandate density-corrected dose calculations.
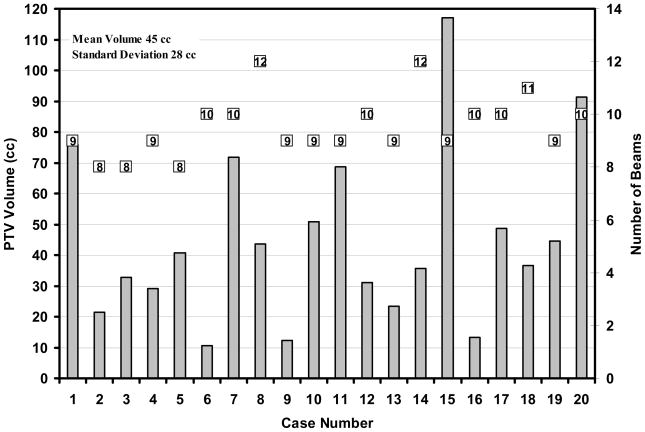
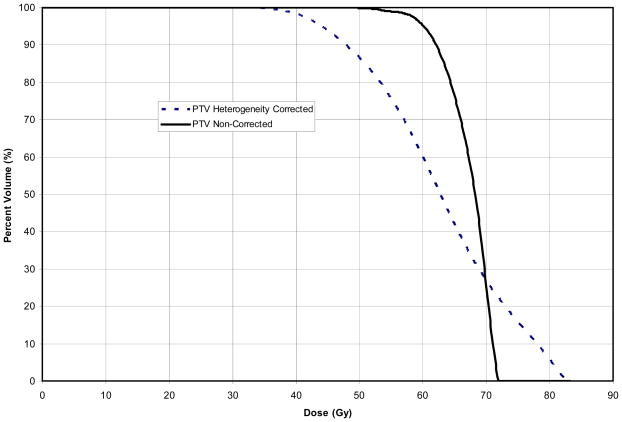
A subset of 20 patients from four institutions participating in the RTOG 0236 protocol and using superposition/convolution algorithms were compared. The RTOG 0236 protocol required a prescription dose of 60 Gy delivered in three fractions to cover 95% of the planning target volume. Additional requirements were specified for target dose heterogeneity and the dose to normal tissue/structures. The protocol required each site to plan the patient's treatment using unit density, and another plan with the same monitor units and applying density corrections was also submitted. These plans were compared to determine the dose differences. Two-sided, paired Student's t tests were used to evaluate these differences.
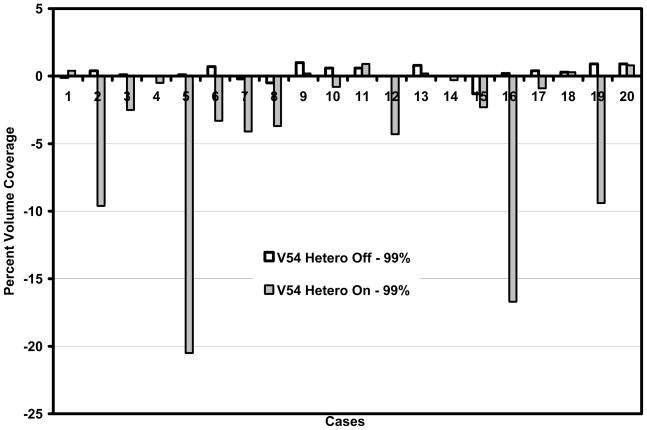
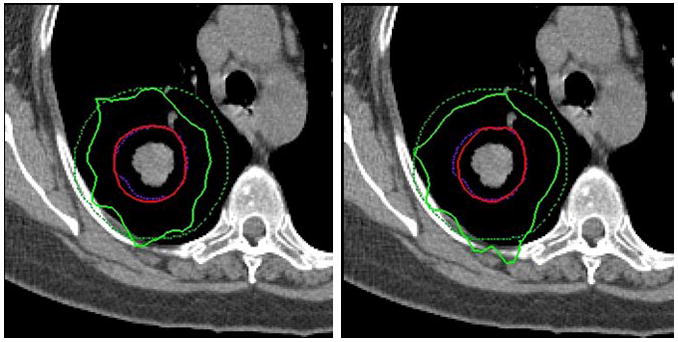
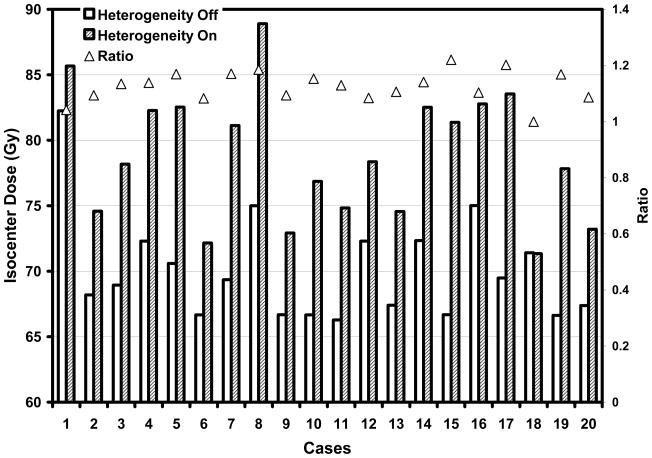
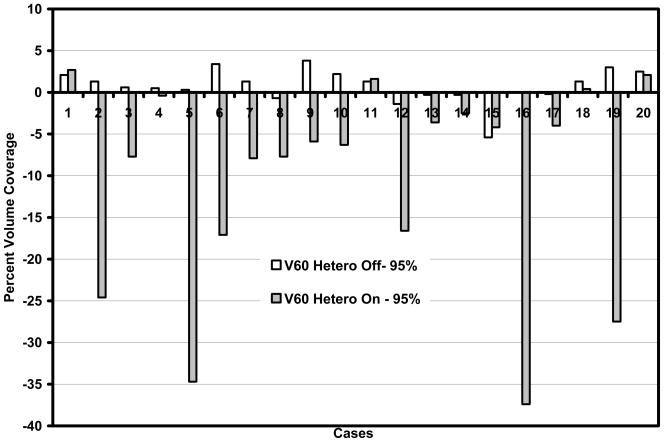
With heterogeneity corrections applied, the planning target volume receiving >/=60 Gy decreased, on average, 10.1% (standard error, 2.7%) from 95% (p = .001). The maximal dose to any point >/=2 cm away from the planning target volume increased from 35.2 Gy (standard error, 1.7) to 38.5 Gy (standard error, 2.2).
Statistically significant dose differences were found with the heterogeneity corrections. The information provided in the present study is being used to design future heterogeneity-corrected RTOG stereotactic body radiotherapy lung protocols to match the true dose delivered for RTOG 0236.
通过对多个向放射治疗肿瘤学组(RTOG)0236非小细胞立体定向体部放射治疗方案招募患者的机构提交的治疗计划进行回顾性分析,本研究确定了未来要求进行密度校正剂量计算的立体定向体部放射治疗肺部方案的剂量处方和关键结构限制。
比较了来自四个参与RTOG 0236方案并使用叠加/卷积算法的机构的20名患者的子集。RTOG 0236方案要求分三次给予60 Gy的处方剂量,以覆盖95%的计划靶体积。对靶区剂量异质性和正常组织/结构的剂量规定了额外要求。该方案要求每个机构使用单位密度来规划患者的治疗,并且还要提交一个具有相同监测单位并应用密度校正的计划。比较这些计划以确定剂量差异。使用双侧配对t检验来评估这些差异。
应用异质性校正后,接受≥60 Gy的计划靶体积平均从95%下降了10.1%(标准误差,2.7%)(p = 0.001)。距离计划靶体积≥2 cm的任何点的最大剂量从35.2 Gy(标准误差,1.7)增加到38.5 Gy(标准误差,2.2)。
发现异质性校正存在统计学上显著的剂量差异。本研究提供的信息正用于设计未来经异质性校正后的RTOG立体定向体部放射治疗肺部方案,以匹配RTOG 0236实际给予的剂量。