Brown Joshua B, Cohen Mitchell J, Minei Joseph P, Maier Ronald V, West Michaela A, Billiar Timothy R, Peitzman Andrew B, Moore Ernest E, Cuschieri Joseph, Sperry Jason L
*Division of General Surgery and Trauma, Department of Surgery, University of Pittsburgh Medical Center, Pittsburgh, PA †Department of Surgery, University of California, San Francisco, CA ‡Division of Burn, Trauma, Critical Care, Department of Surgery, University of Texas Southwestern Medical Center, Dallas, TX §Division of General Surgery and Trauma, Harborview Medical Center, and the Department of Surgery, University of Washington, Seattle, WA; and ‖Department of Surgery, Denver Health Medical Center, and The University of Colorado Health Sciences Center, Denver, CO.
Ann Surg. 2015 May;261(5):997-1005. doi: 10.1097/SLA.0000000000000674.
To evaluate the association of pretrauma center (PTC) red blood cell (RBC) transfusion with outcomes in severely injured patients.
Hemorrhage remains a major driver of mortality. Little evidence exists supporting PTC interventions to mitigate this.
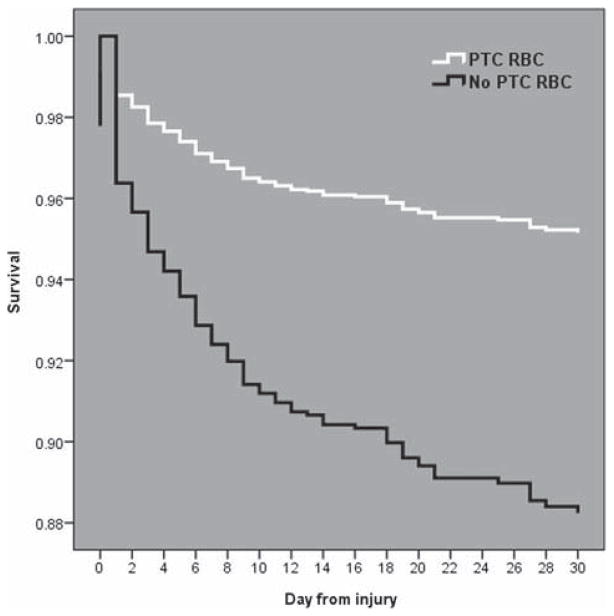
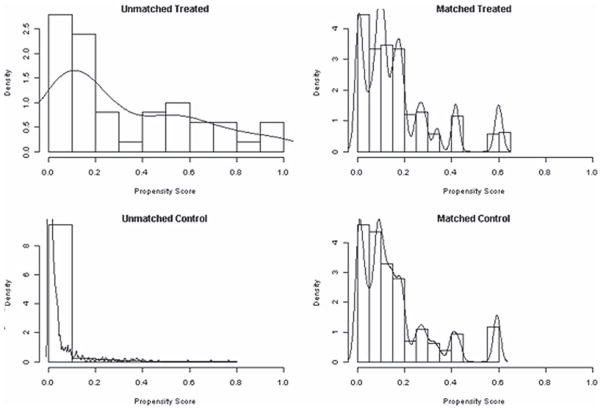
Blunt injured patients in shock arriving at a trauma center within 2 hours of injury were included from the Glue Grant database. Subjects were dichotomized by PTC RBC transfusion. Outcomes included 24-hour mortality, 30-day mortality, and trauma-induced coagulopathy [(TIC), admission international normalized ratio >1.5]. Cox regression and logistic regression determined the association of PTC RBC transfusion with outcomes. To address baseline differences, propensity score matching was used.
Of 1415 subjects, 50 received PTC RBC transfusion. Demographics and injury severity score were similar. The PTC RBC group received 1.3 units of RBCs (median), and 52% were scene transports. PTC RBC transfusion was associated with a 95% reduction in odds of 24-hour mortality [odds ratio (OR) = 0.05; 95% confidence interval (CI), 0.01-0.48; P < 0.01], 64% reduction in the risk of 30-day mortality [hazard ratio = 0.36; 95% CI, 0.15-0.83; P = 0.02], and 88% reduction in odds of TIC (OR = 0.12; 95% CI, 0.02-0.79; P = 0.03). The matched cohort included 113 subjects (31% PTC RBC group). Baseline characteristics were similar. PTC RBC transfusion was associated with a 98% reduction in odds of 24-hour mortality (OR = 0.02; 95% CI, 0.01-0.69; P = 0.04), 88% reduction in the risk of 30-day mortality (hazard ratio = 0.12; 95% CI, 0.03-0.61; P = 0.01), and 99% reduction in odds of TIC (OR = 0.01; 95% CI, 0.01-0.95; P = 0.05).
PTC RBC administration was associated with a lower risk of 24-hour mortality, 30-day mortality, and TIC in severely injured patients with blunt trauma, warranting further prospective study.
评估创伤中心前(PTC)红细胞(RBC)输注与重伤患者预后之间的关联。
出血仍然是死亡的主要原因。几乎没有证据支持PTC干预措施来减轻这一情况。
从胶水基金数据库中纳入受伤后2小时内到达创伤中心的钝性损伤休克患者。根据PTC红细胞输注情况将受试者分为两组。结局指标包括24小时死亡率、30天死亡率和创伤性凝血病(TIC,入院国际标准化比值>1.5)。Cox回归和逻辑回归确定PTC红细胞输注与结局之间的关联。为解决基线差异,采用倾向得分匹配法。
在1415名受试者中,50名接受了PTC红细胞输注。人口统计学和损伤严重程度评分相似。PTC红细胞组输注了1.3单位红细胞(中位数),52%为现场转运。PTC红细胞输注与24小时死亡率的几率降低95%相关[比值比(OR)=0.05;95%置信区间(CI),0.01 - 0.48;P<0.01],30天死亡率风险降低64%[风险比=0.36;95%CI,0.15 - 0.83;P = 0.02],TIC几率降低88%(OR = 0.12;95%CI,0.02 - 0.79;P = 0.03)。匹配队列包括113名受试者(PTC红细胞组占31%)。基线特征相似。PTC红细胞输注与24小时死亡率的几率降低98%相关(OR = 0.02;95%CI,0.01 - 0.69;P = 0.04),30天死亡率风险降低88%(风险比=0.12;95%CI,0.03 - 0.61;P = 0.01),TIC几率降低99%(OR = 0.01;95%CI,0.01 - 0.95;P = 0.05)。
在钝性创伤的重伤患者中,PTC红细胞输注与24小时死亡率、30天死亡率和TIC风险较低相关,值得进一步进行前瞻性研究。