Department of Clinical Oncology, Leeds Cancer Centre, St. James's University Hospital, Leeds, United Kingdom; University of Leeds, Leeds, United Kingdom.
Department of Medical Physics, Leeds Cancer Centre, St. James's University Hospital, Leeds, United Kingdom.
Int J Radiat Oncol Biol Phys. 2014 Jun 1;89(2):406-15. doi: 10.1016/j.ijrobp.2014.01.042. Epub 2014 Mar 28.
To investigate boosting dominant intraprostatic lesions (DILs) in the context of stereotactic ablative radiation therapy (SABR) and to examine the impact on tumor control probability (TCP) and normal tissue complication probability (NTCP).
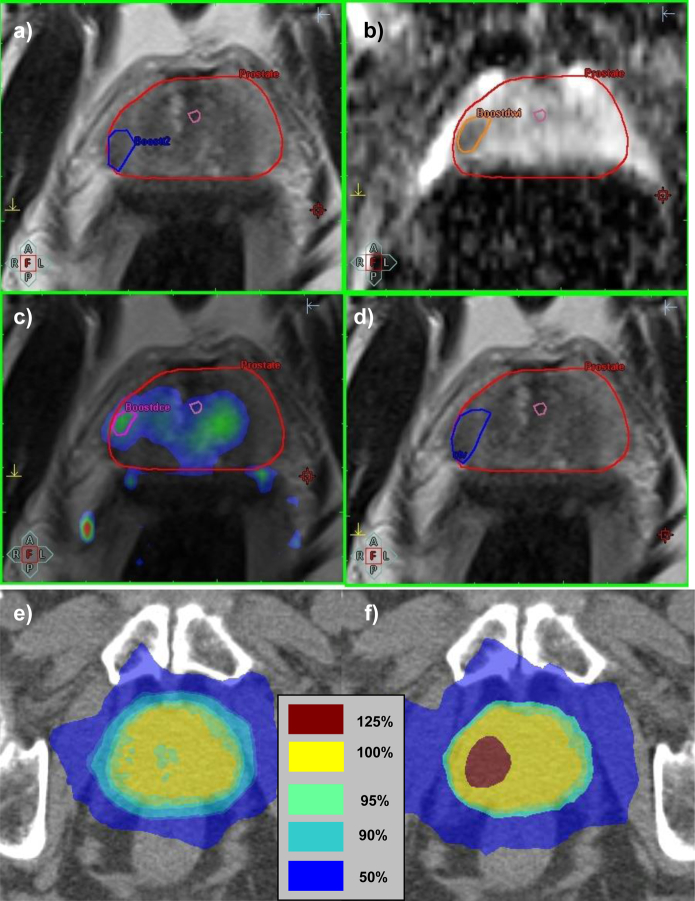
Ten prostate datasets were selected. DILs were defined using T2-weighted, dynamic contrast-enhanced and diffusion-weighted magnetic resonance imaging. Four plans were produced for each dataset: (1) no boost to DILs; (2) boost to DILs, no seminal vesicles in prescription; (3) boost to DILs, proximal seminal vesicles (proxSV) prescribed intermediate dose; and (4) boost to DILs, proxSV prescribed higher dose. The prostate planning target volume (PTV) prescription was 42.7 Gy in 7 fractions. DILs were initially prescribed 115% of the PTV(Prostate) prescription, and PTV(DIL) prescriptions were increased in 5% increments until organ-at-risk constraints were reached. TCP and NTCP calculations used the LQ-Poisson Marsden, and Lyman-Kutcher-Burman models respectively.
When treating the prostate alone, the median PTV(DIL) prescription was 125% (range: 110%-140%) of the PTV(Prostate) prescription. Median PTV(DIL) D50% was 55.1 Gy (range: 49.6-62.6 Gy). The same PTV(DIL) prescriptions and similar PTV(DIL) median doses were possible when including the proxSV within the prescription. TCP depended on prostate α/β ratio and was highest with an α/β ratio = 1.5 Gy, where the additional TCP benefit of DIL boosting was least. Rectal NTCP increased with DIL boosting and was considered unacceptably high in 5 cases, which, when replanned with an emphasis on reducing maximum dose to 0.5 cm(3) of rectum (Dmax(0.5cc)), as well as meeting existing constraints, resulted in considerable rectal NTCP reductions.
Boosting DILs in the context of SABR is technically feasible but should be approached with caution. If this therapy is adopted, strict rectal constraints are required including Dmax(0.5cc). If the α/β ratio of prostate cancer is 1.5 Gy or less, then high TCP and low NTCP can be achieved by prescribing SABR to the whole prostate, without the need for DIL boosting.
在立体定向消融放疗(SABR)的背景下研究增强优势前列腺内病变(DIL),并探讨其对肿瘤控制概率(TCP)和正常组织并发症概率(NTCP)的影响。
选择了 10 个前列腺数据集。使用 T2 加权、动态对比增强和弥散加权磁共振成像来定义 DIL。为每个数据集生成了 4 个计划:(1)不向 DIL 施加增强;(2)向 DIL 施加增强,但不在处方中包含精囊;(3)向 DIL 施加增强,同时对近端精囊(proxSV)给予中剂量处方;(4)向 DIL 施加增强,同时对 proxSV 给予高剂量处方。前列腺计划靶区(PTV)的处方剂量为 7 次分割的 42.7 Gy。DIL 的初始处方剂量为 PTV(Prostate)处方的 115%,然后以 5%的增量增加 PTV(DIL)的处方剂量,直到达到危及器官的限制。TCP 和 NTCP 的计算分别使用 LQ-Poisson Marsden 和 Lyman-Kutcher-Burman 模型。
当单独治疗前列腺时,PTV(DIL)的中位处方剂量为 PTV(Prostate)处方的 125%(范围:110%-140%)。PTV(DIL)D50%的中位数为 55.1 Gy(范围:49.6-62.6 Gy)。当将 proxSV 包含在处方中时,也可以采用相同的 PTV(DIL)处方和类似的 PTV(DIL)中位剂量。TCP 取决于前列腺的 α/β 比值,当 α/β 比值为 1.5 Gy 时,TCP 最高,而 DIL 增强的额外 TCP 获益最小。直肠 NTCP 随 DIL 增强而增加,在 5 例中被认为过高,当重新规划时,重点是将直肠最大剂量(Dmax(0.5cc))降低至 0.5 cm(3)直肠,并满足现有限制,直肠 NTCP 显著降低。
在 SABR 的背景下,增强 DIL 在技术上是可行的,但应谨慎采用。如果采用这种治疗方法,则需要严格的直肠限制,包括 Dmax(0.5cc)。如果前列腺癌的 α/β 比值为 1.5 Gy 或更低,则通过向整个前列腺进行 SABR 治疗,可以实现高 TCP 和低 NTCP,而无需增强 DIL。