Jespersen Lasse, Abildstrom Steen Z, Hvelplund Anders, Madsen Jan K, Galatius Soren, Pedersen Frants, Hojberg Soren, Prescott Eva
Department of Cardiology, Bispebjerg University Hospital, Copenhagen, Denmark.
National Institute of Public Health, University of Southern Denmark, Copenhagen, Denmark; Department of Cardiology, Gentofte University Hospital, Hellerup, Denmark.
PLoS One. 2014 Apr 4;9(4):e93170. doi: 10.1371/journal.pone.0093170. eCollection 2014.
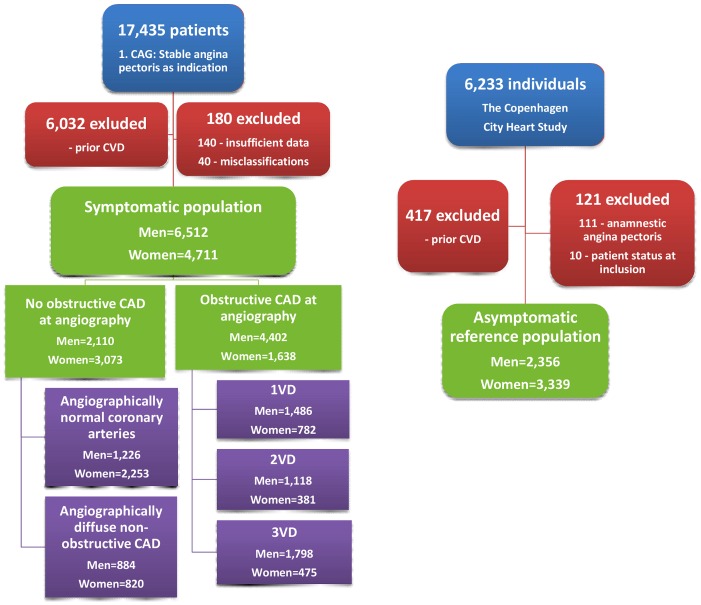
To evaluate risk of hospitalization due to cardiovascular disease (CVD) and repeat coronary angiography (CAG) in stable angina pectoris (SAP) with no obstructive coronary artery disease (CAD) versus obstructive CAD, and asymptomatic reference individuals.
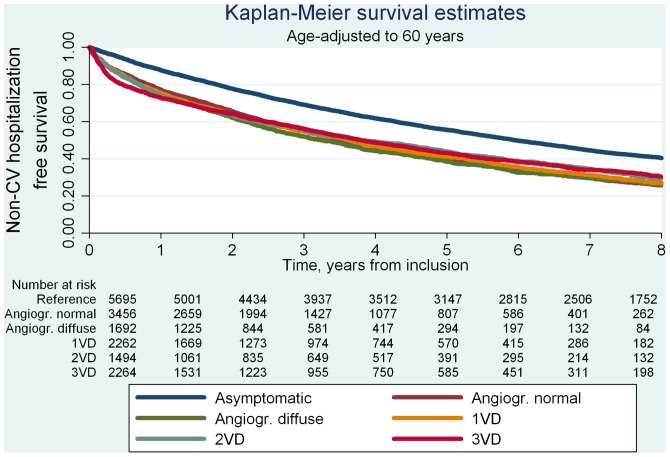
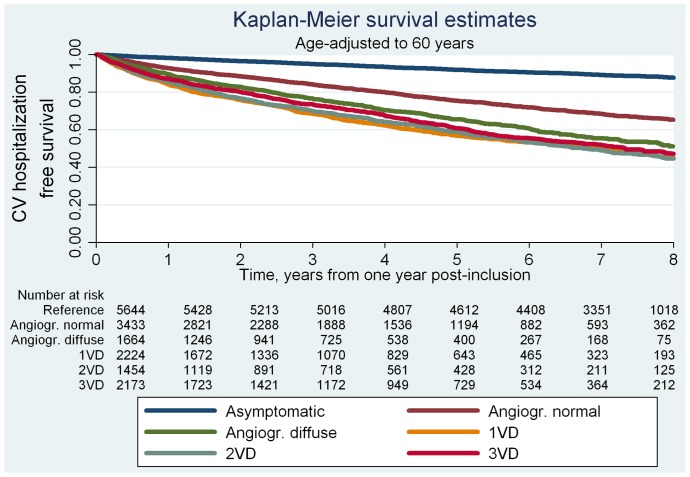
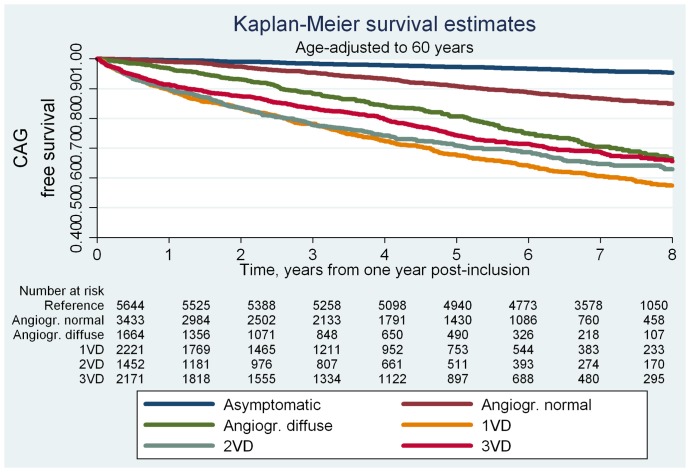
We followed 11,223 patients with no prior CVD having a first-time CAG in 1998-2009 due to SAP symptoms and 5,695 asymptomatic reference individuals from the Copenhagen City Heart Study through registry linkage for 7.8 years (median). In recurrent event survival analysis, patients with SAP had 3-4-fold higher risk of hospitalization for CVD irrespective of CAG findings and cardiovascular comorbidity. Multivariable adjusted hazard ratios(95%CI) for patients with angiographically normal coronary arteries was 3.0(2.5-3.5), for angiographically diffuse non-obstructive CAD 3.9(3.3-4.6) and for 1-3-vessel disease 3.6-4.1(range)(all P<0.001). Mean accumulated hospitalization time was 3.5(3.0-4.0)(days/10 years follow-up) in reference individuals and 4.5(3.8-5.2)/7.0(5.4-8.6)/6.7(5.2-8.1)/6.1(5.2-7.4)/8.6(6.6-10.7) in patients with angiographically normal coronary arteries/angiographically diffuse non-obstructive CAD/1-, 2-, and 3-vessel disease, respectively (all P<0.05, age-adjusted). SAP symptoms predicted repeat CAG with multivariable adjusted hazard ratios for patients with angiographically normal coronary arteries being 2.3(1.9-2.9), for angiographically diffuse non-obstructive CAD 5.5(4.4-6.8) and for obstructive CAD 6.6-9.4(range)(all P<0.001).
Patients with SAP symptoms and angiographically normal coronary arteries or angiographically diffuse non-obstructive CAD suffer from considerably greater CVD burdens in terms of hospitalization for CVD and repeat CAG compared with asymptomatic reference individuals even after adjustment for cardiac risk factors and exclusion of cardiovascular comorbidity as cause. Contrary to common perception, excluding obstructive CAD by CAG in such patients does not ensure a benign cardiovascular prognosis.
评估无阻塞性冠状动脉疾病(CAD)的稳定型心绞痛(SAP)患者与阻塞性CAD患者以及无症状对照个体因心血管疾病(CVD)住院和重复冠状动脉造影(CAG)的风险。
我们对1998 - 2009年因SAP症状首次进行CAG且既往无CVD的11223例患者以及哥本哈根市心脏研究中的5695例无症状对照个体进行了7.8年(中位数)的登记链接随访。在复发事件生存分析中,无论CAG结果和心血管合并症如何,SAP患者因CVD住院的风险高出3 - 4倍。冠状动脉造影正常的患者多变量调整后的风险比(95%CI)为3.0(2.5 - 3.5),冠状动脉造影弥漫性非阻塞性CAD患者为3.9(3.3 - 4.6),1 - 3支血管病变患者为3.6 - 4.1(范围)(均P<0.001)。对照个体的平均累计住院时间为3.5(3.0 - 4.0)(天/10年随访),冠状动脉造影正常的患者为4.5(3.8 - 5.2)/7.0(5.4 - 8.6)/6.7(5.2 - 8.1)/6.1(5.2 - 7.4)/8.6(6.6 - 10.7),分别对应冠状动脉造影弥漫性非阻塞性CAD/1、2和3支血管病变患者(均P<0.05,年龄调整后)。SAP症状可预测重复CAG,冠状动脉造影正常的患者多变量调整后的风险比为2.3(1.9 - 2.9),冠状动脉造影弥漫性非阻塞性CAD患者为5.5(4.4 - 6.8),阻塞性CAD患者为6.6 - 9.4(范围)(均P<0.001)。
有SAP症状且冠状动脉造影正常或冠状动脉造影弥漫性非阻塞性CAD的患者,即使在调整心脏危险因素并排除心血管合并症为病因后,与无症状对照个体相比,在因CVD住院和重复CAG方面承受着相当大的CVD负担。与普遍看法相反,在此类患者中通过CAG排除阻塞性CAD并不能确保良好的心血管预后。