Partin Alan W, Van Neste Leander, Klein Eric A, Marks Leonard S, Gee Jason R, Troyer Dean A, Rieger-Christ Kimberly, Jones J Stephen, Magi-Galluzzi Cristina, Mangold Leslie A, Trock Bruce J, Lance Raymond S, Bigley Joseph W, Van Criekinge Wim, Epstein Jonathan I
James Buchanan Brady Urological Institute, The Johns Hopkins University School of Medicine, Baltimore, Maryland.
Department of Pathology, GROW School for Oncology and Developmental Biology, Maastricht University Medical Center, Maastricht, The Netherlands; MDxHealth, Inc., Irvine, California.
J Urol. 2014 Oct;192(4):1081-7. doi: 10.1016/j.juro.2014.04.013. Epub 2014 Apr 18.
The DOCUMENT multicenter trial in the United States validated the performance of an epigenetic test as an independent predictor of prostate cancer risk to guide decision making for repeat biopsy. Confirming an increased negative predictive value could help avoid unnecessary repeat biopsies.
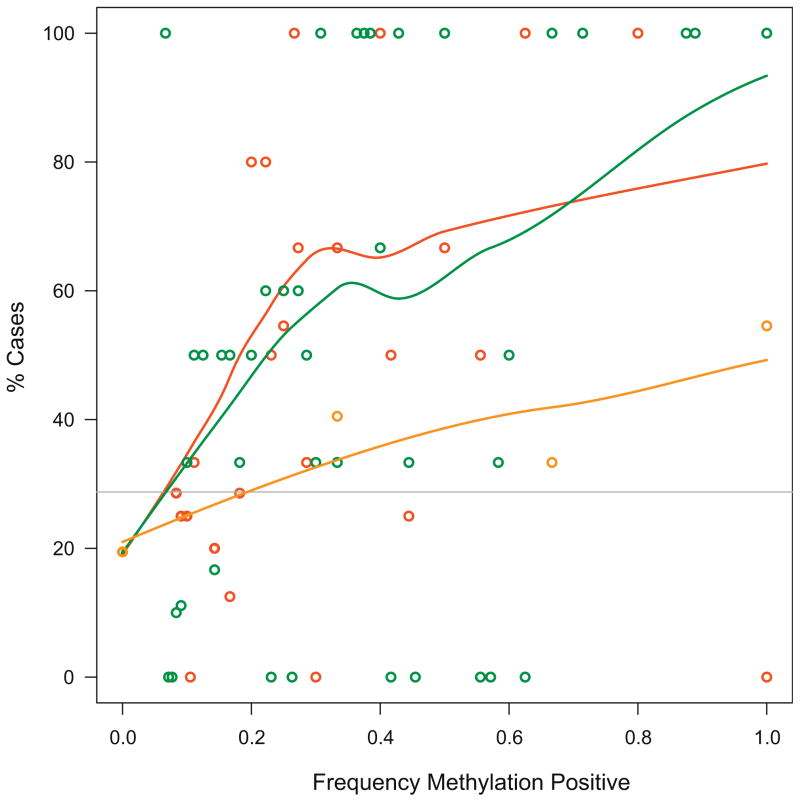
We evaluated the archived, cancer negative prostate biopsy core tissue samples of 350 subjects from a total of 5 urological centers in the United States. All subjects underwent repeat biopsy within 24 months with a negative (controls) or positive (cases) histopathological result. Centralized blinded pathology evaluation of the 2 biopsy series was performed in all available subjects from each site. Biopsies were epigenetically profiled for GSTP1, APC and RASSF1 relative to the ACTB reference gene using quantitative methylation specific polymerase chain reaction. Predetermined analytical marker cutoffs were used to determine assay performance. Multivariate logistic regression was used to evaluate all risk factors.
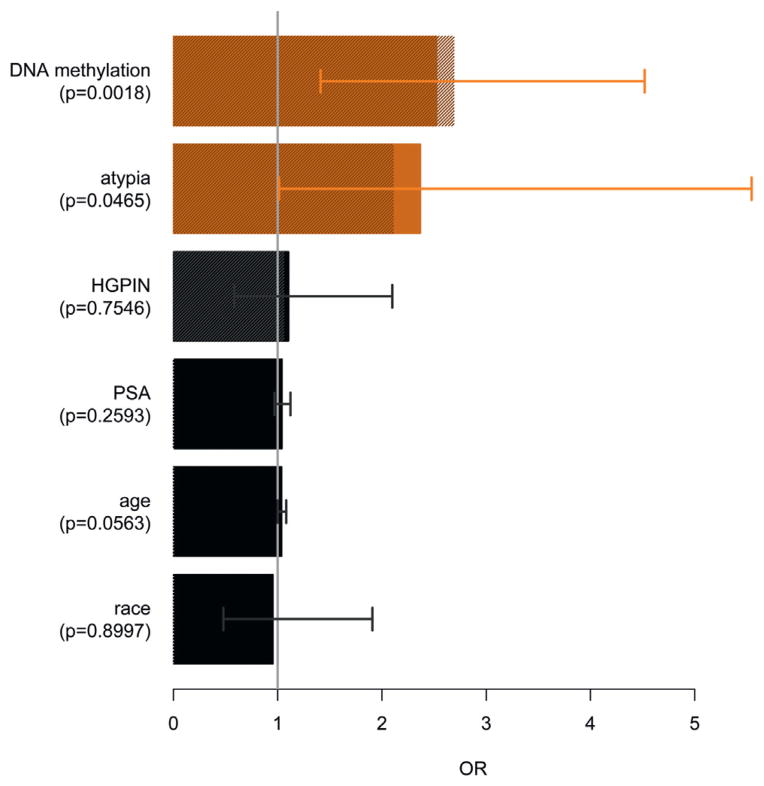
The epigenetic assay resulted in a negative predictive value of 88% (95% CI 85-91). In multivariate models correcting for age, prostate specific antigen, digital rectal examination, first biopsy histopathological characteristics and race the test proved to be the most significant independent predictor of patient outcome (OR 2.69, 95% CI 1.60-4.51).
The DOCUMENT study validated that the epigenetic assay was a significant, independent predictor of prostate cancer detection in a repeat biopsy collected an average of 13 months after an initial negative result. Due to its 88% negative predictive value adding this epigenetic assay to other known risk factors may help decrease unnecessary repeat prostate biopsies.
美国的多中心试验验证了一种表观遗传学检测作为前列腺癌风险独立预测指标的性能,以指导重复活检的决策制定。确认阴性预测值增加有助于避免不必要的重复活检。
我们评估了来自美国5个泌尿外科中心的350名受试者的存档、癌症阴性前列腺活检核心组织样本。所有受试者在24个月内进行了重复活检,组织病理学结果为阴性(对照组)或阳性(病例组)。对每个部位所有可用受试者的2个活检系列进行集中盲法病理评估。使用定量甲基化特异性聚合酶链反应,相对于ACTB参考基因,对活检样本进行GSTP1、APC和RASSF1的表观遗传学分析。使用预定的分析标志物临界值来确定检测性能。采用多变量逻辑回归评估所有风险因素。
表观遗传学检测的阴性预测值为88%(95%可信区间85-91)。在校正年龄、前列腺特异性抗原、直肠指检、首次活检组织病理学特征和种族的多变量模型中,该检测被证明是患者预后的最显著独立预测指标(比值比2.69,95%可信区间1.60-4.51)。
DOCUMENT研究验证了表观遗传学检测是在首次阴性结果后平均13个月采集的重复活检中前列腺癌检测的重要独立预测指标。由于其88%的阴性预测值,将这种表观遗传学检测添加到其他已知风险因素中可能有助于减少不必要的重复前列腺活检。