Johansson Emily White, Gething Peter W, Hildenwall Helena, Mappin Bonnie, Petzold Max, Peterson Stefan Swartling, Selling Katarina Ekholm
International Maternal and Child Health, Department of Women's and Children's Health, Uppsala University, Uppsala, Sweden.
Spatial Ecology and Epidemiology Group, Department of Zoology, University of Oxford, Oxford, United Kingdom.
PLoS One. 2014 Apr 18;9(4):e95483. doi: 10.1371/journal.pone.0095483. eCollection 2014.
In 2010, the World Health Organization revised guidelines to recommend diagnosis of all suspected malaria cases prior to treatment. There has been no systematic assessment of malaria test uptake for pediatric fevers at the population level as countries start implementing guidelines. We examined test use for pediatric fevers in relation to malaria endemicity and treatment-seeking behavior in multiple sub-Saharan African countries in initial years of implementation.
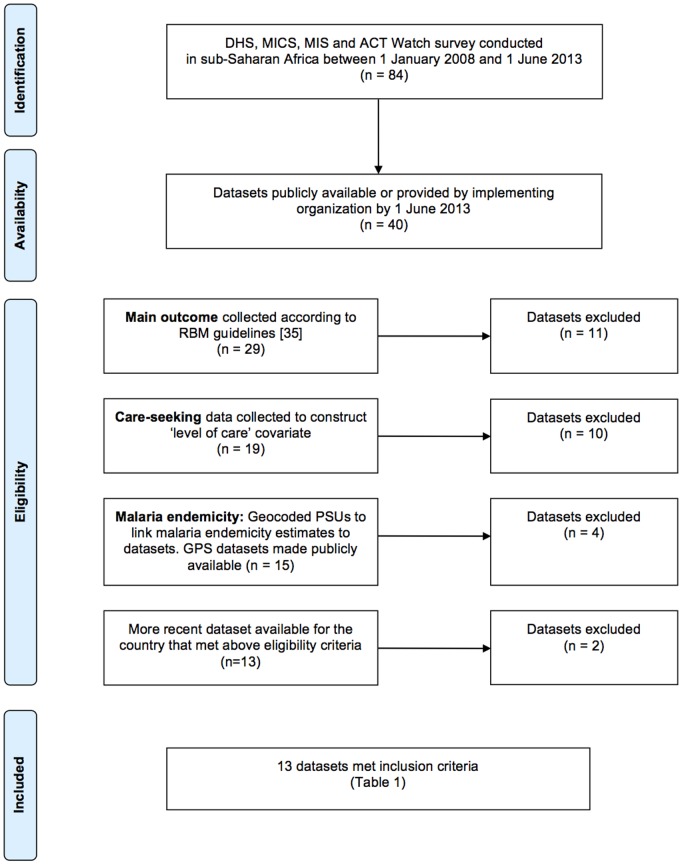
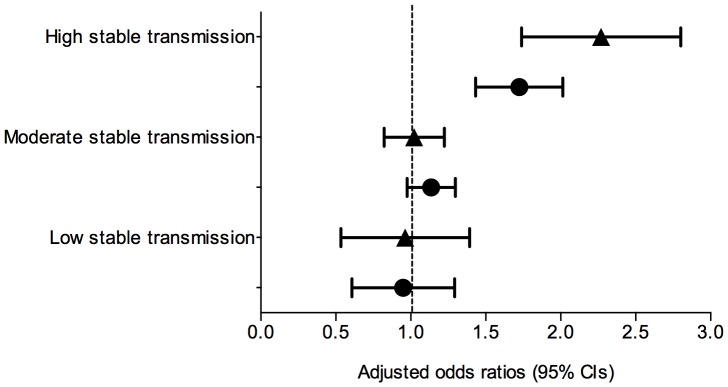
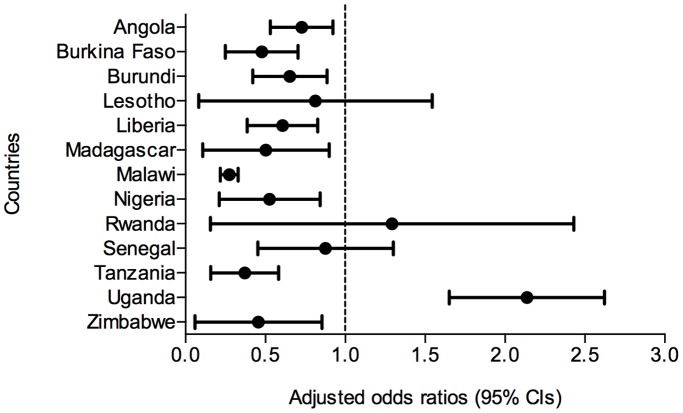
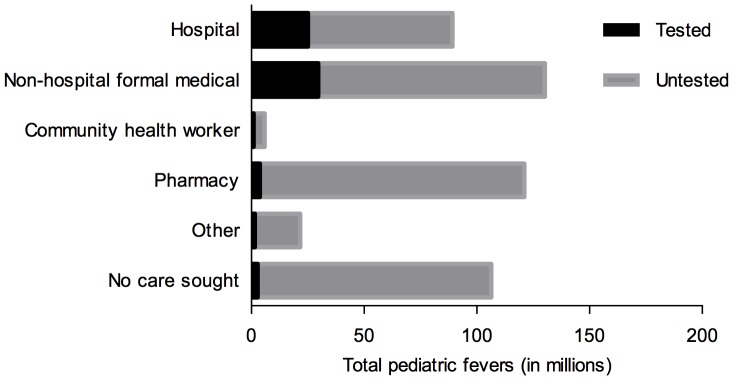
We compiled data from national population-based surveys reporting fever prevalence, care-seeking and diagnostic use for children under five years in 13 sub-Saharan African countries in 2009-2011/12 (n = 105,791). Mixed-effects logistic regression models quantified the influence of source of care and malaria endemicity on test use after adjusting for socioeconomic covariates. Results were stratified by malaria endemicity categories: low (PfPR2-10<5%), moderate (PfPR2-10 5-40%), high (PfPR2-10>40%). Among febrile under-fives surveyed, 16.9% (95% CI: 11.8%-21.9%) were tested. Compared to hospitals, febrile children attending non-hospital sources (OR: 0.62, 95% CI: 0.56-0.69) and community health workers (OR: 0.31, 95% CI: 0.23-0.43) were less often tested. Febrile children in high-risk areas had reduced odds of testing compared to low-risk settings (OR: 0.51, 95% CI: 0.42-0.62). Febrile children in least poor households were more often tested than in poorest (OR: 1.63, 95% CI: 1.39-1.91), as were children with better-educated mothers compared to least educated (OR: 1.33, 95% CI: 1.16-1.54).
Diagnostic testing of pediatric fevers was low and inequitable at the outset of new guidelines. Greater testing is needed at lower or less formal sources where pediatric fevers are commonly managed, particularly to reach the poorest. Lower test uptake in high-risk settings merits further investigation given potential implications for diagnostic scale-up in these areas. Findings could inform continued implementation of new guidelines to improve access to and equity in point-of-care diagnostics use for pediatric fevers.
2010年,世界卫生组织修订了指南,建议在治疗前对所有疑似疟疾病例进行诊断。随着各国开始实施这些指南,尚未在人群层面系统评估儿科发热患者的疟疾检测率。在实施的最初几年,我们研究了撒哈拉以南非洲多个国家儿科发热检测的使用情况与疟疾流行程度及就医行为之间的关系。
我们汇总了2009 - 2011/12年撒哈拉以南非洲13个国家基于全国人口调查的数据,这些数据报告了五岁以下儿童的发热患病率、就医情况及诊断检测使用情况(n = 105,791)。混合效应逻辑回归模型在调整社会经济协变量后,量化了就医来源和疟疾流行程度对检测使用的影响。结果按疟疾流行程度类别分层:低(PfPR2 - 10 < 5%)、中(PfPR2 - 10 5 - 40%)、高(PfPR2 - 10 > 40%)。在接受调查的发热五岁以下儿童中,16.9%(95%置信区间:11.8% - 21.9%)接受了检测。与医院相比,在非医院机构就诊的发热儿童(比值比:0.62,95%置信区间:0.56 - 0.69)和社区卫生工作者处就诊的发热儿童(比值比:0.31,95%置信区间:0.23 - 0.43)接受检测的频率较低。与低风险地区相比,高风险地区的发热儿童接受检测的几率降低(比值比:0.51,95%置信区间:0.42 - 0.62)。最不贫困家庭的发热儿童接受检测的频率高于最贫困家庭(比值比:1.63,95%置信区间:1.39 - 1.91),母亲受教育程度较高的儿童接受检测的频率高于受教育程度最低的儿童(比值比:1.33,95%置信区间:1.16 - 1.54)。
新指南实施之初,儿科发热的诊断检测率较低且存在不公平现象。在通常管理儿科发热的较低或不太正规的机构需要进行更多检测,特别是要覆盖最贫困人群。鉴于对这些地区扩大诊断规模的潜在影响,高风险地区检测率较低的情况值得进一步调查。研究结果可为持续实施新指南提供参考,以改善儿科发热即时诊断检测的可及性和公平性。