Department of Otorhinolaryngology-Head and Neck Surgery, Osaka University Faculty of Medicine, Suita, Osaka, Japan.
Department of Pathology, Osaka University Faculty of Medicine, Suita, Osaka, Japan.
PLoS One. 2014 Apr 21;9(4):e95364. doi: 10.1371/journal.pone.0095364. eCollection 2014.
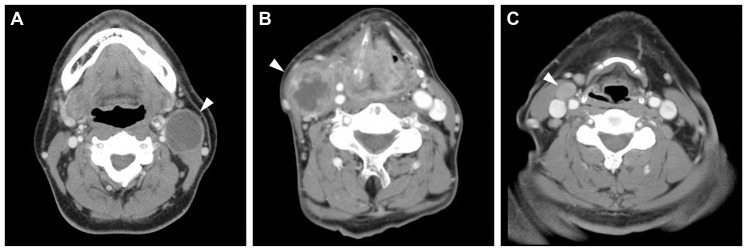
The clinical significance of human papillomavirus (HPV) in neck node metastasis from cancer of unknown primary (CUP) is not well established. We aimed to address the relationship of HPV status between node metastasis and the primary tumor, and also the relevance of HPV status regarding radiographically detected cystic node metastasis in head and neck squamous cell carcinoma (HNSCC) and CUP. HPV DNA was examined in 68 matched pairs of node metastasis and primary tumor, and in node metastasis from 27 CUPs. In surgically treated CUPs, p16 was examined immunohistochemically. When tonsillectomy proved occult tonsillar cancer in CUP, HPV DNA and p16 were also examined in the occult primary. Cystic node metastasis on contrast-enhanced computed tomography scans was correlated with the primary site and HPV status in another series of 255 HNSCCs and CUPs with known HPV status. Node metastasis was HPV-positive in 19/37 (51%) oropharyngeal SCCs (OPSCCs) and 10/27 (37%) CUPs, but not in non-OPSCCs. Fluid was collected from cystic node metastasis using fine needle aspiration in two OPSCCs and one CUP, and all fluid collections were HPV-positive. HPV status, including the presence of HPV DNA, genotype, and physical status, as well as the expression pattern of p16 were consistent between node metastasis and primary or occult primary tumor. Occult tonsillar cancer was found more frequently in p16-positive CUP than in p16-negative CUP (odds ratio (OR), 39.0; 95% confidence interval (CI), 1.4-377.8; P = 0.02). Radiographically, cystic node metastasis was specific to OPSCC and CUP, and was associated with HPV positivity relative to necrotic or solid node metastasis (OR, 6.2; 95% CI, 1.2-45.7; P = 0.03). In conclusion, HPV status remains unchanged after metastasis. The occult primary of HPV-positive CUP is most probably localized in the oropharynx. HPV status determined from fine needle aspirates facilitates the diagnosis of cystic node metastasis.
人乳头瘤病毒 (HPV) 在不明原发灶 (CUP) 颈部淋巴结转移中的临床意义尚未明确。我们旨在研究 HPV 状态与淋巴结转移和原发灶的关系,以及 HPV 状态与头颈部鳞状细胞癌 (HNSCC) 和 CUP 中影像学检测到的囊性淋巴结转移的相关性。在 68 对淋巴结转移和原发肿瘤以及 27 例 CUP 的淋巴结转移中检测了 HPV DNA。在手术治疗的 CUP 中,用免疫组化法检测了 p16。当扁桃体切除术证实 CUP 中有隐匿性扁桃体癌时,也在隐匿性原发灶中检测了 HPV DNA 和 p16。在另一组 255 例已知 HPV 状态的 HNSCC 和 CUP 中,对比增强 CT 扫描显示囊性淋巴结转移与原发部位和 HPV 状态相关。19/37(51%)例口咽鳞癌(OPSCC)和 10/27(37%)例 CUP 的淋巴结转移为 HPV 阳性,而非 OPSCC 则无。在 2 例 OPSCC 和 1 例 CUP 中,使用细针抽吸从囊性淋巴结转移中收集了液体,所有液体采集均为 HPV 阳性。HPV 状态,包括 HPV DNA、基因型和物理状态以及 p16 的表达模式,在淋巴结转移和原发或隐匿性原发肿瘤之间均一致。p16 阳性 CUP 中隐匿性扁桃体癌的检出率高于 p16 阴性 CUP(比值比 (OR),39.0;95%置信区间 (CI),1.4-377.8;P=0.02)。影像学检查显示,囊性淋巴结转移是 OPSCC 和 CUP 的特征,与坏死或实性淋巴结转移相比,与 HPV 阳性相关(OR,6.2;95%CI,1.2-45.7;P=0.03)。总之,HPV 状态转移后保持不变。HPV 阳性 CUP 的隐匿性原发灶最有可能位于口咽。从细针抽吸物中确定 HPV 状态有助于诊断囊性淋巴结转移。