Department of Surgery and Transplantation, Chaim Sheba Medical Center, Tel Aviv University, Israel and Assia Medical Colorectal Group.
Gastroenterol Rep (Oxf). 2014 May;2(2):126-33. doi: 10.1093/gastro/gou008. Epub 2014 Mar 12.
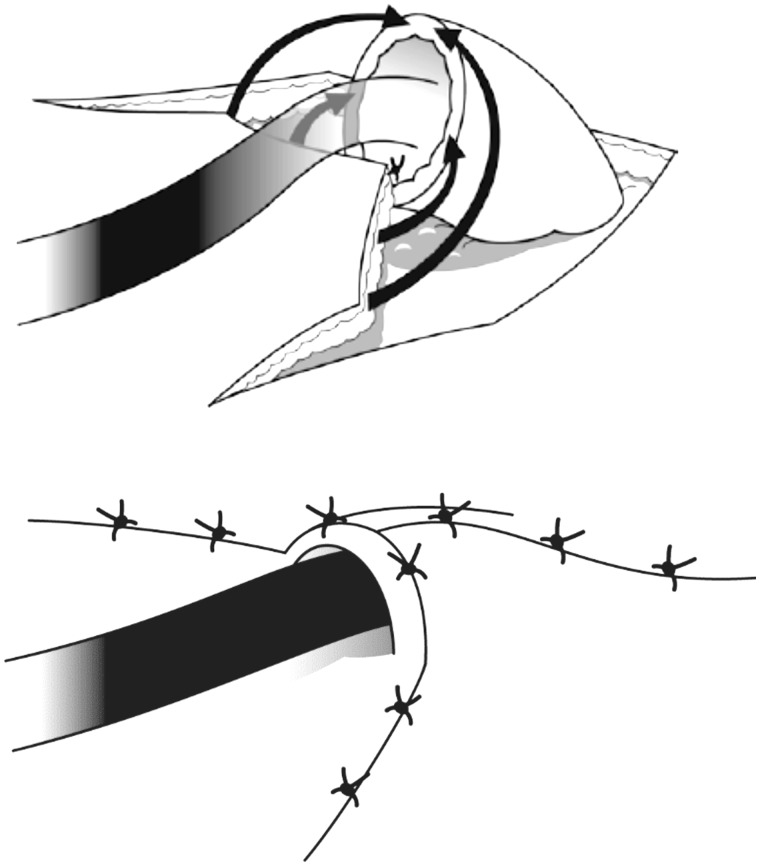
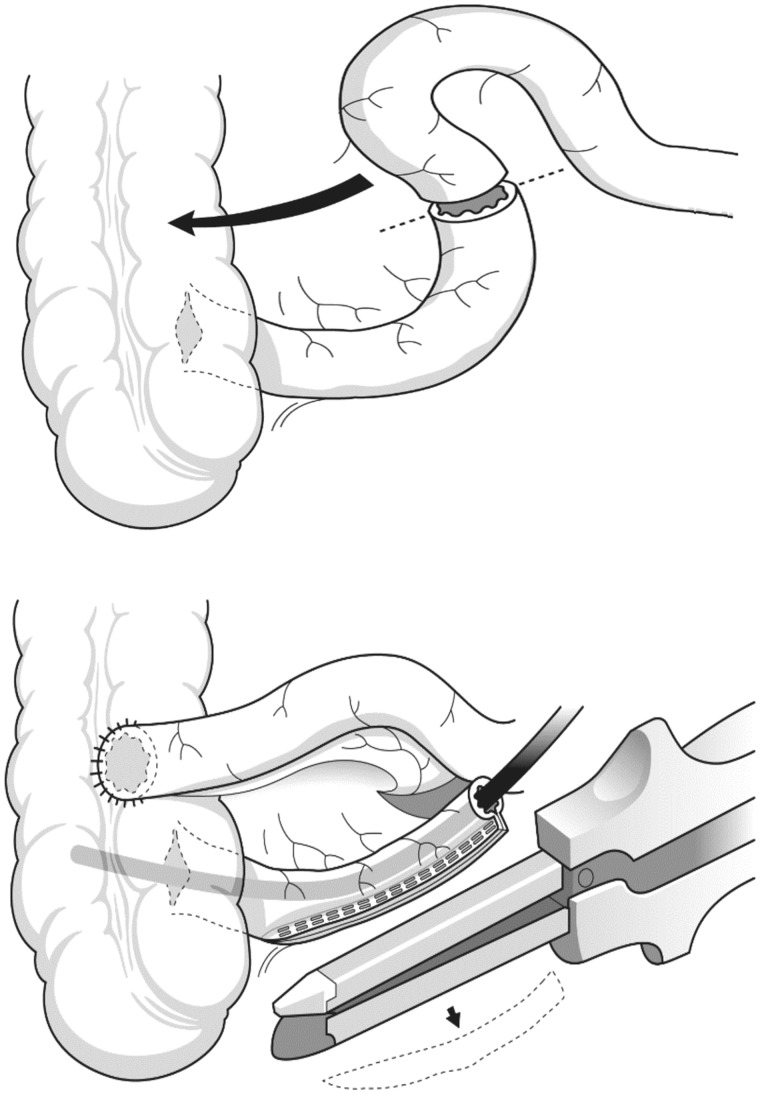
Patients may present with anal incontinence (AI) following repair of a congenital anorectal anomaly years previously, or require total anorectal reconstruction (TAR) following radical rectal extirpation, most commonly for rectal cancer. Others may require removal of their colostomy following sphincter excision for Fournier's gangrene, or in cases of severe perineal trauma. Most of the data pertaining to antegrade continence enema (the ACE or Malone procedure) comes from the pediatric literature in the management of children with AI, but also with supervening chronic constipation, where the quality of life and compliance with this technique appears superior to retrograde colonic washouts. Total anorectal reconstruction requires an anatomical or physical supplement to the performance of a perineal colostomy, which may include an extrinsic muscle interposition (which may or may not be 'dynamized'), construction of a neorectal reservoir, implantation of an incremental artificial bowel sphincter or creation of a terminal, smooth-muscle neosphincter. The advantages and disadvantages of these techniques and their outcome are presented here.
患者可能在多年前修复先天性肛门直肠畸形后出现肛门失禁 (AI),或者在根治性直肠切除术后需要进行全直肠重建 (TAR),最常见的原因是直肠癌。其他人可能需要在因 Fournier 坏疽切除括约肌后,或者在严重会阴创伤的情况下,移除他们的结肠造口。大多数关于经肛门逆行灌洗(ACE 或 Malone 手术)的资料来自于儿科文献,用于治疗患有 AI 且并发慢性便秘的儿童,其生活质量和对该技术的依从性似乎优于逆行结肠灌洗。全直肠重建需要对会阴结肠造口术进行解剖或物理补充,这可能包括外在肌肉插入(可能有或没有“动力化”)、新直肠储袋的构建、增量式人工肠造口括约肌的植入或终端平滑肌肉新括约肌的创建。本文介绍了这些技术的优缺点及其结果。