Gotti Daria, Raffetti Elena, Albini Laura, Sighinolfi Laura, Maggiolo Franco, Di Filippo Elisa, Ladisa Nicoletta, Angarano Gioacchino, Lapadula Giuseppe, Pan Angelo, Esposti Anna Degli, Fabbiani Massimiliano, Focà Emanuele, Scalzini Alfredo, Donato Francesco, Quiros-Roldan Eugenia
University Division of Infectious and Tropical Diseases, University of Brescia, Brescia, Italy.
Section of Hygiene, Epidemiology and Public Health, University of Brescia, Brescia, Italy.
PLoS One. 2014 Apr 23;9(4):e94768. doi: 10.1371/journal.pone.0094768. eCollection 2014.
We studied survival and associated risk factors in an Italian nationwide cohort of HIV-infected individuals after an AIDS-defining cancer (ADC) or non-AIDS-defining cancer (NADC) diagnosis in the modern cART era.
Multi-center, retrospective, observational study of HIV patients included in the MASTER Italian Cohort with a cancer diagnosis from January 1998 to September 2012. Malignancies were divided into ADC or NADC on the basis of the Centre for Disease Control-1993 classification. Recurrence of cancer and metastases were excluded. Survivals were estimated according to the Kaplan-Meier method and compared according to the log-rank test. Statistically significant variables at univariate analysis were entered in a multivariate Cox regression model.
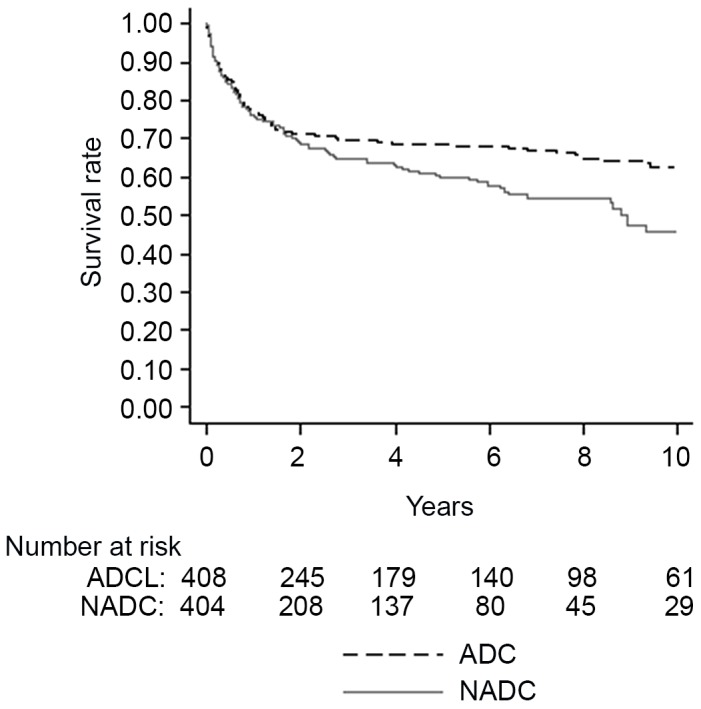
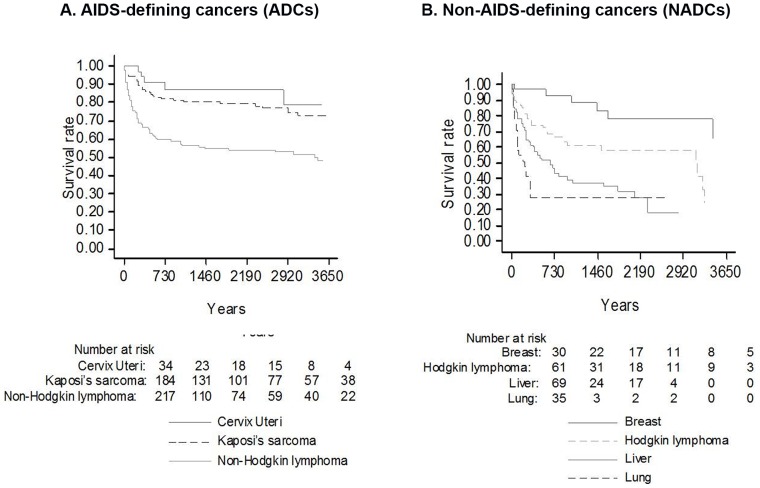
Eight hundred and sixty-six cancer diagnoses were recorded among 13,388 subjects in the MASTER Database after 1998: 435 (51%) were ADCs and 431 (49%) were NADCs. Survival was more favorable after an ADC diagnosis than a NADC diagnosis (10-year survival: 62.7%±2.9% vs. 46%±4.2%; p = 0.017). Non-Hodgkin lymphoma had lower survival rates than patients with Kaposi sarcoma or cervical cancer (10-year survival: 48.2%±4.3% vs. 72.8%±4.0% vs. 78.5%±9.9%; p<0.001). Regarding NADCs, breast cancer showed better survival (10-year survival: 65.1%±14%) than lung cancer (1-year survival: 28%±8.7%), liver cancer (5-year survival: 31.9%±6.4%) or Hodgkin lymphoma (10-year survival: 24.8%±11.2%). Lower CD4+ count and intravenous drug use were significantly associated with decreased survival after ADCs or NADCs diagnosis. Exposure to cART was found to be associated with prolonged survival only in the case of ADCs.
cART has improved survival in patients with an ADC diagnosis, whereas the prognosis after a diagnosis of NADCs is poor. Low CD4+ counts and intravenous drug use are risk factors for survival following a diagnosis of ADCs and Hodgkin lymphoma in the NADC group.
我们研究了现代联合抗逆转录病毒治疗(cART)时代,意大利全国范围内一组感染HIV个体在确诊艾滋病定义的癌症(ADC)或非艾滋病定义的癌症(NADC)后的生存情况及相关风险因素。
对纳入意大利MASTER队列的HIV患者进行多中心、回顾性、观察性研究,这些患者在1998年1月至2012年9月期间被诊断患有癌症。根据疾病控制中心1993年的分类,将恶性肿瘤分为ADC或NADC。排除癌症复发和转移情况。采用Kaplan-Meier方法估计生存率,并通过对数秩检验进行比较。单因素分析中具有统计学意义的变量被纳入多变量Cox回归模型。
1998年后,MASTER数据库中13388名受试者共记录了866例癌症诊断:435例(51%)为ADC,431例(49%)为NADC。ADC诊断后的生存率比NADC诊断后的生存率更有利(10年生存率:62.7%±2.9%对46%±4.2%;p = 0.017)。非霍奇金淋巴瘤的生存率低于卡波西肉瘤或宫颈癌患者(10年生存率:48.2%±4.3%对72.8%±4.0%对78.5%±9.9%;p<0.001)。对于NADC,乳腺癌的生存率(10年生存率:65.1%±14%)高于肺癌(1年生存率:28%±8.7%)、肝癌(5年生存率:31.9%±6.4%)或霍奇金淋巴瘤(10年生存率:24.8%±11.2%)。较低的CD4 +细胞计数和静脉吸毒与ADC或NADC诊断后的生存率降低显著相关。仅在ADC患者中发现接受cART与延长生存期有关。
cART改善了ADC诊断患者的生存率,而NADC诊断后的预后较差。低CD4 +细胞计数和静脉吸毒是ADC诊断后以及NADC组中霍奇金淋巴瘤生存的危险因素。