Worm Signe W, Bower Mark, Reiss Peter, Bonnet Fabrice, Law Matthew, Fätkenheuer Gerd, d'Arminio Monforte Antonella, Abrams Donald I, Grulich Andrew, Fontas Eric, Kirk Ole, Furrer Hansjakob, De Wit Stephane, Phillips Andrew, Lundgren Jens D, Sabin Caroline A
Research Department of Infection and Population Health, University College London, Royal Free Campus, Rowland Hill Street, London NW3 2PF, UK.
BMC Infect Dis. 2013 Oct 9;13:471. doi: 10.1186/1471-2334-13-471.
Non-AIDS defining cancers (NADC) are an important cause of morbidity and mortality in HIV-positive individuals. Using data from a large international cohort of HIV-positive individuals, we described the incidence of NADC from 2004-2010, and described subsequent mortality and predictors of these.
Individuals were followed from 1st January 2004/enrolment in study, until the earliest of a new NADC, 1st February 2010, death or six months after the patient's last visit. Incidence rates were estimated for each year of follow-up, overall and stratified by gender, age and mode of HIV acquisition. Cumulative risk of mortality following NADC diagnosis was summarised using Kaplan-Meier methods, with follow-up for these analyses from the date of NADC diagnosis until the patient's death, 1st February 2010 or 6 months after the patient's last visit. Factors associated with mortality following NADC diagnosis were identified using multivariable Cox proportional hazards regression.
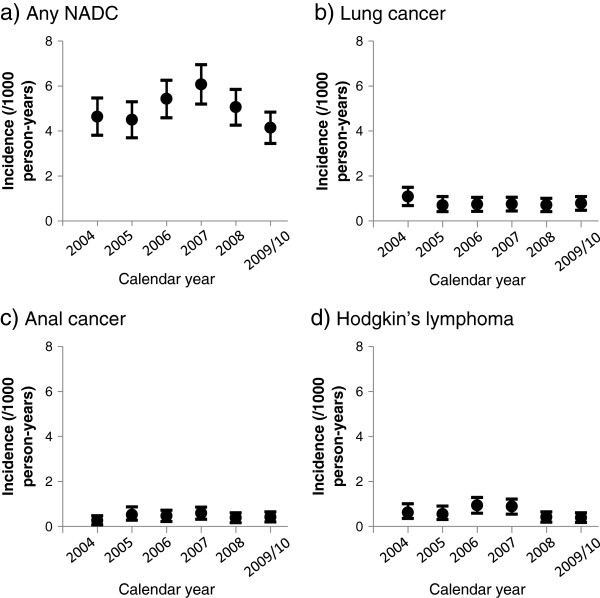
Over 176,775 person-years (PY), 880 (2.1%) patients developed a new NADC (incidence: 4.98/1000PY [95% confidence interval 4.65, 5.31]). Over a third of these patients (327, 37.2%) had died by 1st February 2010. Time trends for lung cancer, anal cancer and Hodgkin's lymphoma were broadly consistent. Kaplan-Meier cumulative mortality estimates at 1, 3 and 5 years after NADC diagnosis were 28.2% [95% CI 25.1-31.2], 42.0% [38.2-45.8] and 47.3% [42.4-52.2], respectively. Significant predictors of poorer survival after diagnosis of NADC were lung cancer (compared to other cancer types), male gender, non-white ethnicity, and smoking status. Later year of diagnosis and higher CD4 count at NADC diagnosis were associated with improved survival. The incidence of NADC remained stable over the period 2004-2010 in this large observational cohort.
The prognosis after diagnosis of NADC, in particular lung cancer and disseminated cancer, is poor but has improved somewhat over time. Modifiable risk factors, such as smoking and low CD4 counts, were associated with mortality following a diagnosis of NADC.
非艾滋病定义性癌症(NADC)是HIV阳性个体发病和死亡的重要原因。利用来自一个大型国际HIV阳性个体队列的数据,我们描述了2004年至2010年NADC的发病率,并描述了随后的死亡率及其预测因素。
对个体从2004年1月1日/研究入组开始进行随访,直至最早出现新的NADC、2010年2月1日、死亡或患者最后一次就诊后6个月。估计每年随访期间的发病率,总体发病率以及按性别、年龄和HIV感染方式分层的发病率。采用Kaplan-Meier方法总结NADC诊断后的累积死亡风险,这些分析的随访时间从NADC诊断日期至患者死亡、2010年2月1日或患者最后一次就诊后6个月。使用多变量Cox比例风险回归确定与NADC诊断后死亡率相关的因素。
在超过176,775人年(PY)的时间里,880名(2.1%)患者出现了新的NADC(发病率:4.98/1000 PY[95%置信区间4.65,5.31])。到2010年2月1日,这些患者中有超过三分之一(327名,37.2%)死亡。肺癌、肛门癌和霍奇金淋巴瘤的时间趋势大致一致。NADC诊断后1年、3年和5年的Kaplan-Meier累积死亡率估计分别为28.2%[95%CI 25.1 - 31.2]、42.0%[38.2 - 45.8]和47.3%[42.4 - 52.2]。NADC诊断后生存较差的显著预测因素是肺癌(与其他癌症类型相比)、男性、非白人种族和吸烟状况。诊断年份较晚以及NADC诊断时CD4计数较高与生存率提高相关。在这个大型观察性队列中,2004年至2010年期间NADC的发病率保持稳定。
NADC诊断后的预后,尤其是肺癌和播散性癌症,较差,但随着时间推移有所改善。可改变的风险因素,如吸烟和低CD4计数,与NADC诊断后的死亡率相关。