Domingo Enric, Grignola Juan C, Aguilar Rio, Arredondo Christian, Bouteldja Nadia, Messeguer Manuel López, Roman Antonio
Pathophysiology Department, School of Medicine, Hospital de Clínicas, Universidad de la República, Avda Italia 2870, PC 11600 Montevideo, Uruguay.
BMC Pulm Med. 2014 Apr 24;14:69. doi: 10.1186/1471-2466-14-69.
Exercise capacity is impaired in pulmonary arterial hypertension (PAH). We hypothesized that cardiovascular reserve abnormalities would be associated with impaired hemodynamic response to pharmacological stress and worse outcome in PAH.
Eighteen PAH patients (p) group 1 NYHA class II/III and ten controls underwent simultaneous right cardiac catheterization and intravascular ultrasound at rest and during low dose-dobutamine (10 mcg/kg/min) with trendelenburg (DST). We estimated cardiac output (CO), pulmonary vascular resistance (PVR) and capacitance (PC), and PA elastic modulus (EM). We concomitantly measured tricuspid annular plane systolic excursion (TAPSE), RV myocardial peak systolic velocity (Sm) and isovolumic myocardial acceleration (IVA) in PAH patients. Based on the rounded mean + 2 SD of the increase in mPAP in our healthy control group during DST (2.8 + 1.8 mm Hg), PAH p were divided into two groups according to mean PA pressure (mPAP) response during DST, 1: ΔmPAP > 5 mm Hg and 2: ΔmPAP ≤ 5 mm Hg. Cardiovascular reserve was estimated as the change (delta, Δ) during DST compared with rest, including ΔmPAP with respect to ΔCO (ΔmPAP/ΔCO). All patients were prospectively followed up for 2 years.
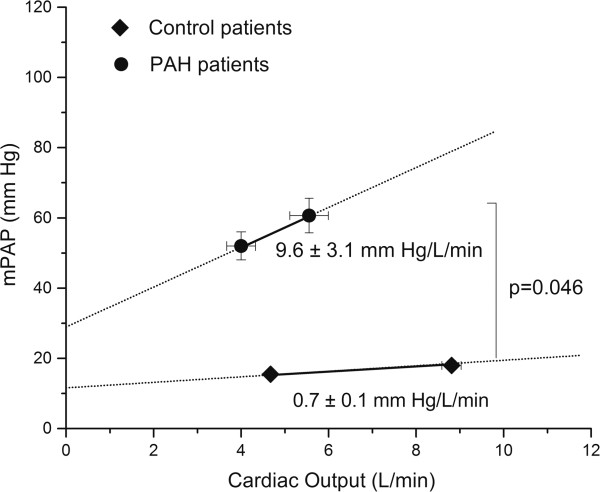
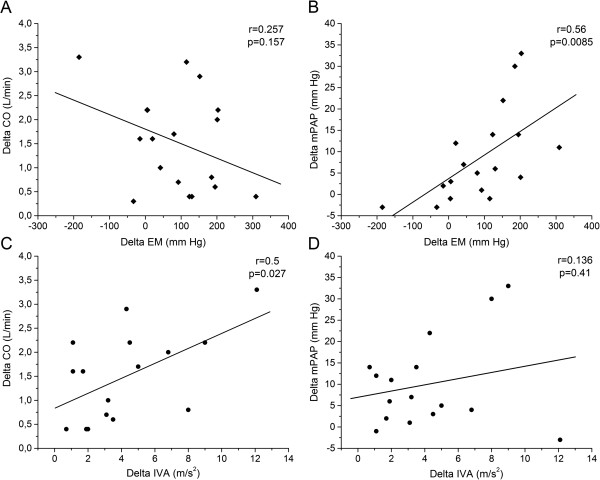
PAH p showed significant lower heart rate and CO increase than controls during DST, with a significant mPAP and pulse PAP increase and higher ΔmPAP/ΔCO (p < 0.05). Neither hemodynamic, IVUS and echocardiographic data were different between both PAH groups at rest. In group 1, DST caused a higher ΔEM, ΔmPAP/ΔCO, ΔPVR, and ΔTAPSE than group 2, with a lower IVA increase and a negative ΔSV (p < 0.05). TAPSE correlated with mPAP and RVP (p < 0.05) and, IVA and Sm correlated with CO (p < 0.05). ΔEM correlated with ΔmPAP and ΔIVA with ΔCO (p < 0.05). There were two deaths/pulmonary transplantations in group 1 and one death in group 2 during the follow-up (p > 0.05).
Pulmonary vascular reserve and RV systolic reserve are significantly impaired in patients with PAH. The lower recruitable cardiovascular reserve is significantly related to a worse hemodynamic response to DST and it could be associated with a poor clinical outcome.
肺动脉高压(PAH)患者的运动能力受损。我们假设心血管储备异常与PAH患者对药物应激的血流动力学反应受损及预后较差有关。
18例PAH患者(第1组,纽约心脏协会II/III级)和10例对照者在静息状态下以及在低剂量多巴酚丁胺(10 mcg/kg/min)联合头低脚高位(DST)期间同时进行右心导管检查和血管内超声检查。我们评估了心输出量(CO)、肺血管阻力(PVR)和容量(PC)以及肺动脉弹性模量(EM)。同时,我们测量了PAH患者的三尖瓣环平面收缩期位移(TAPSE)、右室心肌峰值收缩速度(Sm)和等容心肌加速度(IVA)。根据我们健康对照组在DST期间平均肺动脉压(mPAP)升高的均值+2标准差(2.8 + 1.8 mmHg),PAH患者根据DST期间的平均PA压力(mPAP)反应分为两组:1:ΔmPAP > 5 mmHg和2:ΔmPAP ≤ 5 mmHg。心血管储备通过与静息状态相比DST期间的变化(增量,Δ)来评估,包括相对于ΔCO的ΔmPAP(ΔmPAP/ΔCO)。所有患者均进行了为期2年的前瞻性随访。
PAH患者在DST期间心率和CO的升高显著低于对照组,mPAP和脉压PAP显著升高,且ΔmPAP/ΔCO更高(p < 0.05)。两组PAH患者在静息状态下的血流动力学、血管内超声和超声心动图数据均无差异。在第1组中,DST引起的ΔEM、ΔmPAP/ΔCO、ΔPVR和ΔTAPSE高于第2组,IVA升高较低且ΔSV为负(p < 0.05)。TAPSE与mPAP和右室压力(RVP)相关(p < 0.05),IVA和Sm与CO相关(p < 0.05)。ΔEM与ΔmPAP相关,ΔIVA与ΔCO相关(p < 0.05)。随访期间,第1组有2例死亡/肺移植,第2组有1例死亡(p > 0.05)。
PAH患者的肺血管储备和右室收缩储备显著受损。可募集的心血管储备较低与对DST的血流动力学反应较差显著相关,并且可能与不良临床结局有关。