van den Bos Willemien, Beriwal Sushil, Velema Laura, de Leeuw Astrid A C, Nomden Christel N, Jürgenliemk-Schulz Ina-M
Department of Radiation Oncology, University Medical Center Utrecht, Utrecht, The Netherlands.
Department of Radiation Oncology, University of Pittsburgh Cancer Institute, Pittsburgh, PA, USA.
J Contemp Brachytherapy. 2014 Mar;6(1):21-7. doi: 10.5114/jcb.2014.42021. Epub 2014 Apr 3.
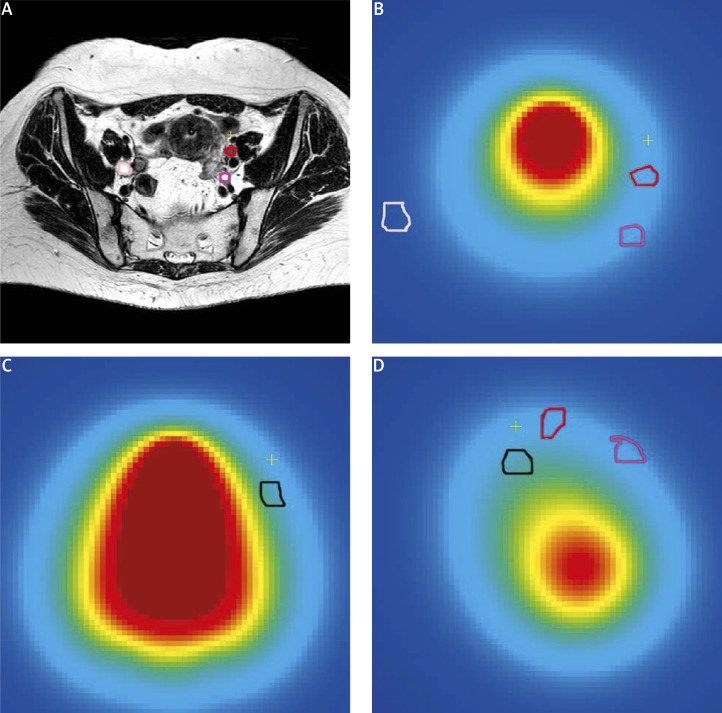
The goal of this study was to determine the dose contributions from image guided adaptive brachytherapy (IGABT) to individual suspicious pelvic lymph nodes (pLNN) in cervical cancer patients. Data were collected in two cancer centers, University of Pittsburgh Cancer Institute (UPCI) and University Medical Center Utrecht (UMCU).
27 and 15 patients with node positive cervical cancer treated with HDR (high dose rate) or PDR (pulsed dose rate)-IGABT were analyzed. HDR-IGABT (UPCI) was delivered with CT/MRI compatible tandem-ring applicators with 5.0-6.0 Gy × five fractions. PDR-IGABT (UMCU) dose was delivered with Utrecht tandem-ovoid applicators with 32 × 0.6 Gy × two fractions. Pelvic lymph nodes with short axis diameter of ≥ 5 mm on pre-treatment MRI or PET-CT were contoured for all BT-plans. Dose contributions to individual pLNN expressed as D90 (dose to 90% of the volume) were calculated from dose-volume histograms as absolute and relative physical dose (% of the reference dose) for each fraction. For each node, the total dose from all fractions was calculated, expressed in EQD2 (equivalent total dose in 2 Gy fractions).
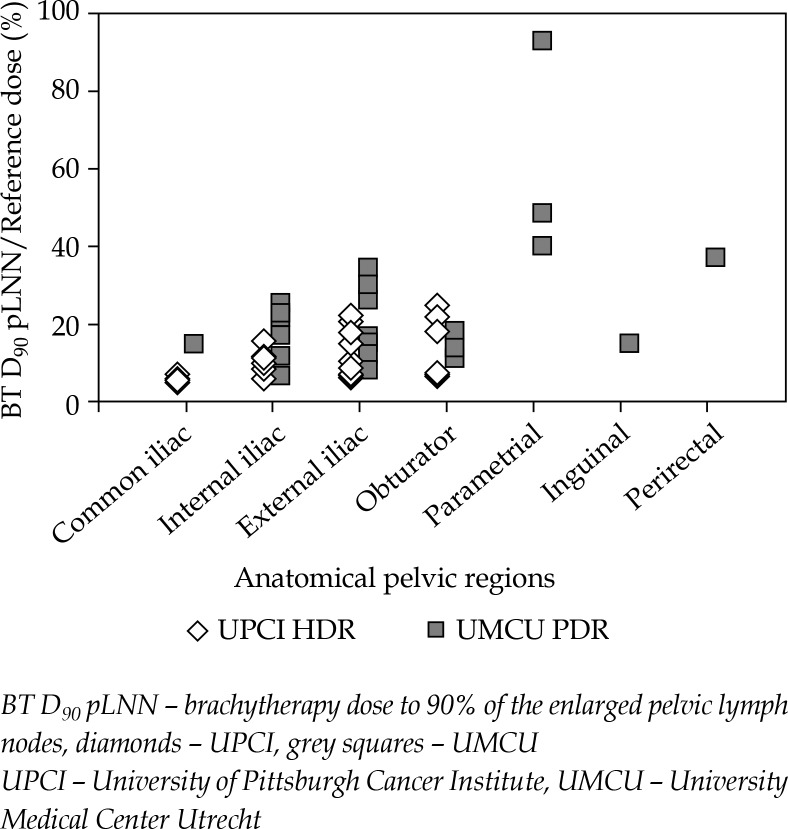
Fifty-seven (UPCI) and 40 (UMCU) individual pLNN were contoured. The mean D90 pLNN was 10.8% (range 5.7-25.1%) and 20.5% (range 6.8-93.3%), respectively, and therefore different in the two centers. These values translate into 2.7 Gy (1.3-6.6 Gy) EQD2 and 7.1 Gy (2.2-36.7 Gy) EQD2, respectively. Differences are caused by the location of the individual nodes in relation to the spatial dose distribution of IGABT, differences in total dose administered and radiobiology (HDR versus PDR).
The IGABT dose contribution to individual pelvic nodes depends on patient and treatment related factors, and varies considerably.
本研究的目的是确定影像引导下的自适应近距离放射治疗(IGABT)对宫颈癌患者个体可疑盆腔淋巴结(pLNN)的剂量贡献。数据收集于两个癌症中心,匹兹堡大学癌症研究所(UPCI)和乌得勒支大学医学中心(UMCU)。
分析了27例和15例接受高剂量率(HDR)或脉冲剂量率(PDR)-IGABT治疗的淋巴结阳性宫颈癌患者。HDR-IGABT(UPCI)采用与CT/MRI兼容的串联环施源器,给予5.0 - 6.0 Gy×5次分割。PDR-IGABT(UMCU)剂量采用乌得勒支串联椭圆体施源器,给予32×0.6 Gy×2次分割。对所有近距离放射治疗计划,在治疗前MRI或PET-CT上对短轴直径≥5 mm的盆腔淋巴结进行轮廓勾画。根据剂量体积直方图计算每个分割中对个体pLNN的剂量贡献,以D90(90%体积的剂量)表示,作为绝对和相对物理剂量(参考剂量的%)。对于每个淋巴结,计算所有分割的总剂量,以EQD2(2 Gy分割的等效总剂量)表示。
共勾画了57个(UPCI)和40个(UMCU)个体pLNN。pLNN的平均D90分别为10.8%(范围5.7 - 25.1%)和20.5%(范围6.8 - 93.3%),因此两个中心不同。这些值分别转化为2.7 Gy(1.3 - 6.6 Gy)EQD2和7.1 Gy(2.2 - 36.7 Gy)EQD2。差异是由个体淋巴结相对于IGABT空间剂量分布的位置、给予的总剂量以及放射生物学(HDR与PDR)的差异引起的。
IGABT对个体盆腔淋巴结的剂量贡献取决于患者和治疗相关因素,且差异很大。