Bonner Carissa, Jansen Jesse, Newell Ben R, Irwig Les, Glasziou Paul, Doust Jenny, Dhillon Haryana, McCaffery Kirsten
Screening and Test Evaluation Program (STEP), Sydney School of Public Health, The University of Sydney, Sydney, Australia.
J Med Internet Res. 2014 May 5;16(5):e120. doi: 10.2196/jmir.3190.
Health risk calculators are widely available on the Internet, including cardiovascular disease (CVD) risk calculators that estimate the probability of a heart attack, stroke, or death over a 5- or 10-year period. Some calculators convert this probability to "heart age", where a heart age older than current age indicates modifiable risk factors. These calculators may impact patient decision making about CVD risk management with or without clinician involvement, but little is known about how patients use them. Previous studies have not investigated patient understanding of heart age compared to 5-year percentage risk, or the best way to present heart age.
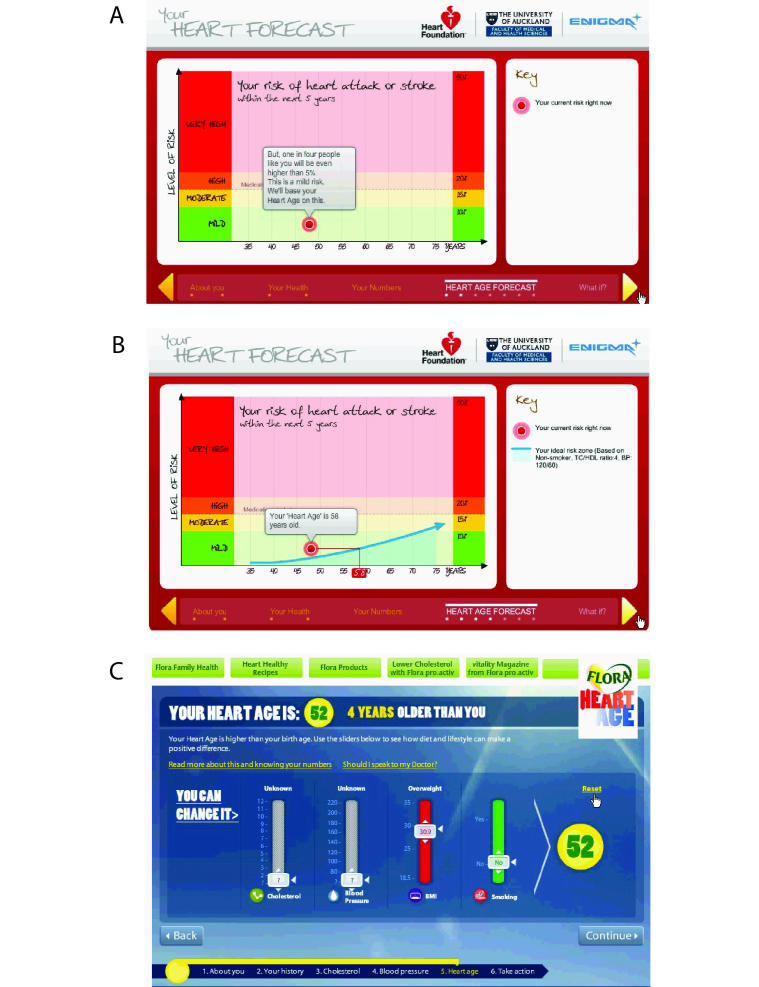
This study aimed to investigate patient experiences and understanding of online heart age calculators that use different verbal, numerical, and graphical formats, based on 5- and 10-year Framingham risk equations used in clinical practice guidelines around the world.
General practitioners in New South Wales, Australia, recruited 26 patients with CVD/lifestyle risk factors who were not taking cholesterol or blood pressure-lowering medication in 2012. Participants were asked to "think aloud" while using two heart age calculators in random order, with semi-structured interviews before and after. Transcribed audio recordings were coded and a framework analysis method was used.
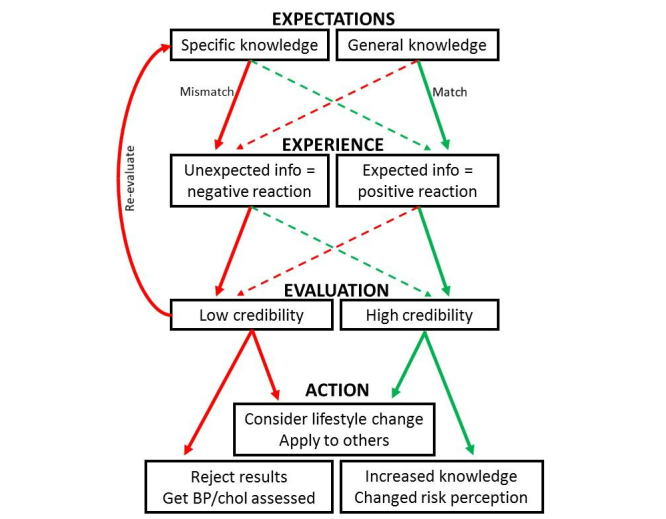
Risk factor questions were often misinterpreted, reducing the accuracy of the calculators. Participants perceived older heart age as confronting and younger heart age as positive but unrealistic. Unexpected or contradictory results (eg, low percentage risk but older heart age) led participants to question the credibility of the calculators. Reasons to discredit the results included the absence of relevant lifestyle questions and impact of corporate sponsorship. However, the calculators prompted participants to consider lifestyle changes irrespective of whether they received younger, same, or older heart age results.
Online heart age calculators can be misunderstood and disregarded if they produce unexpected or contradictory results, but they may still motivate lifestyle changes. Future research should investigate both the benefits and harms of communicating risk in this way, and how to increase the reliability and credibility of online health risk calculators.
健康风险计算器在互联网上广泛可得,包括心血管疾病(CVD)风险计算器,可估算5年或10年内心脏病发作、中风或死亡的概率。一些计算器将此概率转换为“心脏年龄”,心脏年龄大于实际年龄表明存在可改变的风险因素。这些计算器可能会影响患者在有无临床医生参与情况下对CVD风险管理的决策,但对于患者如何使用它们却知之甚少。先前的研究尚未调查患者对心脏年龄与5年风险百分比的理解,以及呈现心脏年龄的最佳方式。
本研究旨在基于全球临床实践指南中使用的5年和10年弗明汉风险方程,调查患者对使用不同语言、数字和图形格式的在线心脏年龄计算器的体验和理解。
2012年,澳大利亚新南威尔士州的全科医生招募了26名有CVD/生活方式风险因素且未服用胆固醇或降压药物的患者。参与者被要求按随机顺序使用两个心脏年龄计算器时“边想边说”,前后进行半结构化访谈。对转录的音频记录进行编码,并采用框架分析方法。
风险因素问题常被误解,降低了计算器的准确性。参与者认为心脏年龄较大令人不安,而心脏年龄较小则是积极的但不现实。意外或矛盾的结果(如低风险百分比但心脏年龄较大)导致参与者质疑计算器的可信度。质疑结果的原因包括缺乏相关生活方式问题以及企业赞助的影响。然而,这些计算器促使参与者考虑生活方式的改变,无论他们得到的心脏年龄结果是更年轻、相同还是更老。
如果在线心脏年龄计算器产生意外或矛盾的结果,可能会被误解和忽视,但它们仍可能促使生活方式的改变。未来的研究应调查以这种方式传达风险的益处和危害,以及如何提高在线健康风险计算器的可靠性和可信度。