Gedik Nilgün, Thielmann Matthias, Kottenberg Eva, Peters Jürgen, Jakob Heinz, Heusch Gerd, Kleinbongard Petra
Institut für Pathophysiologie, Universitätsklinikum Essen, Universität Duisburg-Essen, Essen, Germany.
Klinik für Thorax- und Kardiovaskuläre Chirurgie, Universitätsklinikum Essen, Universität Duisburg-Essen, Essen, Germany.
PLoS One. 2014 May 5;9(5):e96567. doi: 10.1371/journal.pone.0096567. eCollection 2014.
Remote ischemic preconditioning (RIPC) by repeated brief limb ischemia/reperfusion reduces myocardial injury in patients undergoing coronary artery bypass grafting (CABG). Activation of signal transducer and activator of transcription 5 (STAT5) in left ventricular (LV) myocardium at early reperfusion is associated with such protection. Autophagy, i.e., removal of dysfunctional cellular components through lysosomes, has been proposed as one mechanism of cardioprotection. Therefore, we analyzed whether or not the protection by RIPC is associated with activated autophagy.
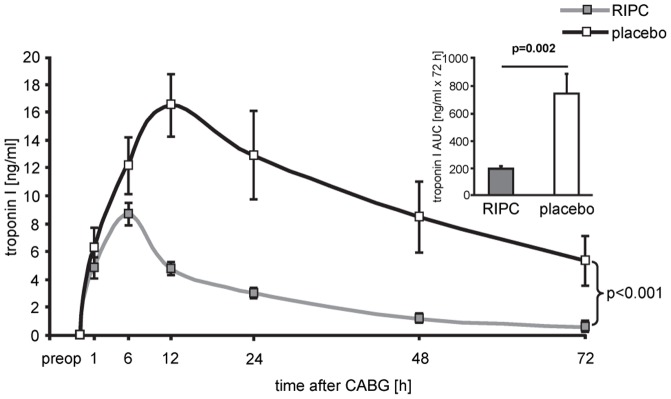
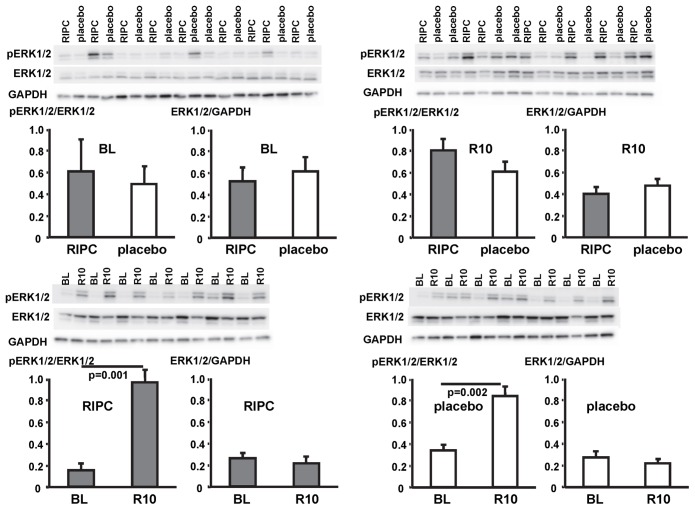
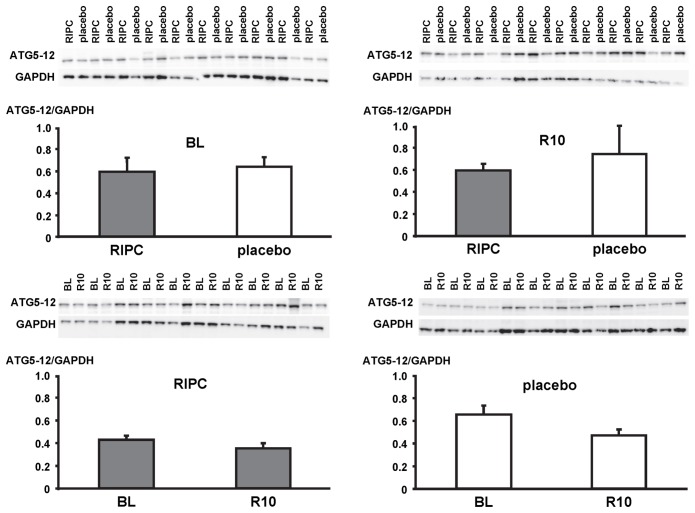
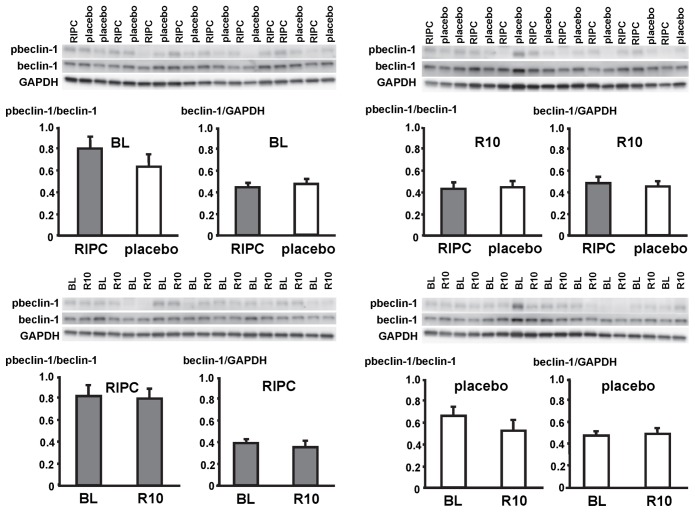
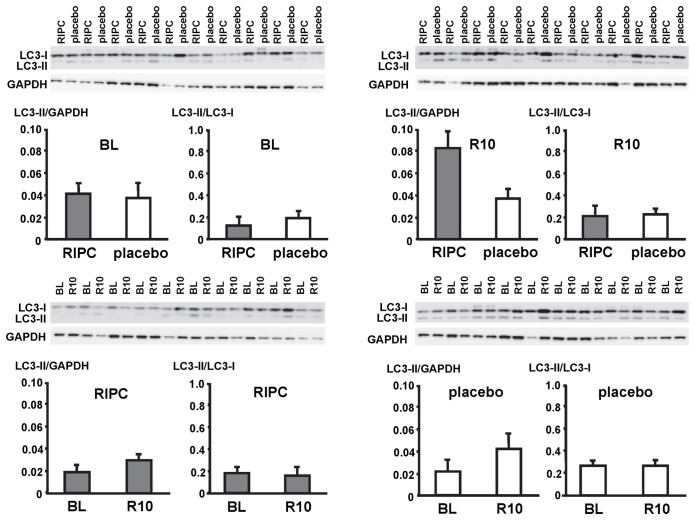
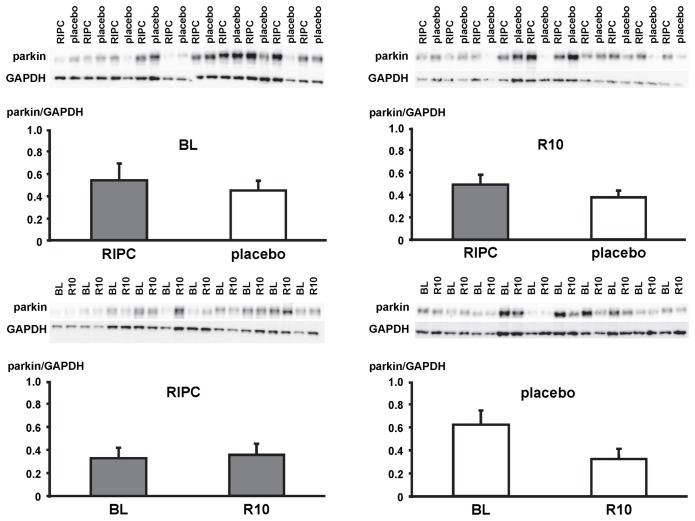
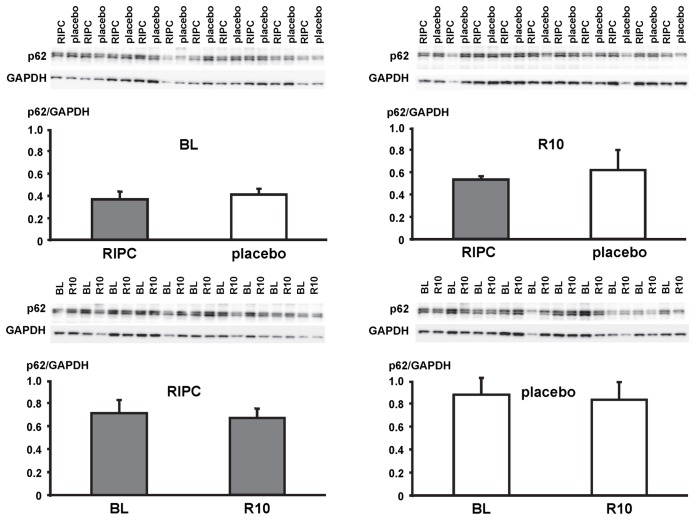
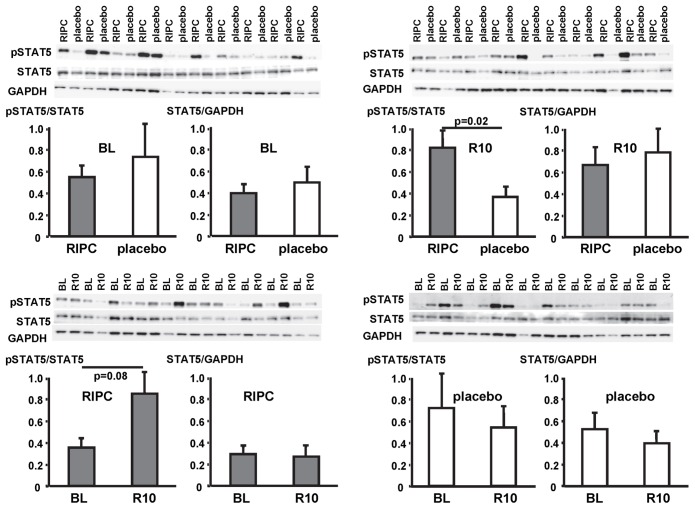
CABG patients were randomized to undergo RIPC (3×5 min blood pressure cuff inflation/5 min deflation) or placebo (cuff deflated) before skin incision (n = 10/10). Transmural myocardial biopsies were taken from the LV before cardioplegia (baseline) and at early (5-10 min) reperfusion. RIPC-induced protection was reflected by decreased serum troponin I concentration area under the curve (194±17 versus 709±129 ng/ml × 72 h, p = 0.002). Western blotting for beclin-1-phosphorylation and protein expression of autophagy-related gene 5-12 (ATG5-12) complex, light chain 3 (LC3), parkin, and p62 was performed. STAT3-, STAT5- and extracellular signal-regulated protein kinase 1/2 (ERK1/2)-phosphorylation was used as positive control to confirm signal activation by ischemia/reperfusion.
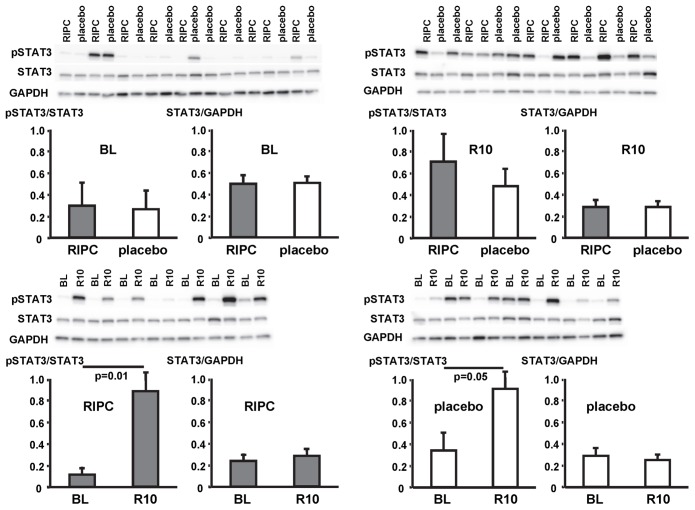
Signals of all analyzed autophagy proteins did not differ between baseline and early reperfusion and not between RIPC and placebo. STAT5-phosphorylation was greater at early reperfusion only with RIPC (2.2-fold, p = 0.02). STAT3- and ERK1/2-phosphorylation were greater at early reperfusion with placebo and RIPC (≥2.7-fold versus baseline, p≤0.05).
Protection through RIPC in patients undergoing CABG surgery does not appear to be associated with enhanced autophagy in LV myocardium at early reperfusion.
通过反复短暂的肢体缺血/再灌注进行的远程缺血预处理(RIPC)可减轻接受冠状动脉旁路移植术(CABG)患者的心肌损伤。再灌注早期左心室(LV)心肌中信号转导和转录激活因子5(STAT5)的激活与这种保护作用相关。自噬,即通过溶酶体清除功能失调的细胞成分,已被提出作为一种心脏保护机制。因此,我们分析了RIPC的保护作用是否与激活的自噬相关。
CABG患者在皮肤切开前被随机分为接受RIPC(3×5分钟血压袖带充气/5分钟放气)或安慰剂(袖带放气)组(n = 10/10)。在心脏停搏前(基线)和早期(5 - 10分钟)再灌注时从左心室获取透壁心肌活检组织。RIPC诱导的保护作用通过血清肌钙蛋白I浓度曲线下面积的降低来反映(194±17对709±129 ng/ml×72小时,p = 0.002)。进行了针对beclin-1磷酸化以及自噬相关基因5 - 12(ATG5 - 12)复合物、轻链3(LC3)、帕金蛋白和p62蛋白表达的蛋白质印迹分析。将STAT3、STAT5和细胞外信号调节蛋白激酶1/2(ERK1/2)的磷酸化作为阳性对照,以确认缺血/再灌注引起的信号激活。
所有分析的自噬蛋白信号在基线和早期再灌注之间以及RIPC组和安慰剂组之间均无差异。仅在RIPC组中,再灌注早期STAT5磷酸化程度更高(2.2倍,p = 0.02)。在安慰剂组和RIPC组中,再灌注早期STAT3和ERK1/2磷酸化程度更高(比基线增加≥2.7倍,p≤0.05)。
在接受CABG手术的患者中,RIPC的保护作用似乎与再灌注早期左心室心肌自噬增强无关。