Miedema Michael D, Duprez Daniel A, Misialek Jeffrey R, Blaha Michael J, Nasir Khurram, Silverman Michael G, Blankstein Ron, Budoff Matthew J, Greenland Philip, Folsom Aaron R
From the Minneapolis Heart Institute and Minneapolis Heart Institute Foundation, Minneapolis, MN (M.D.M.); Brigham and Women's Hospital and Boston VA Healthcare System, Harvard Medical School, Boston, MA (M.D.M.); Cardiovascular Division, University of Minnesota, Minneapolis (D.A.D.); Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis (J.R.M., A.R.F.); Ciccarone Preventive Cardiology Center, Johns Hopkins School of Medicine, Baltimore, MD (M.J.B., K.N., M.G.S.); Center for Prevention and Wellness Research, Baptist Health South Florida, Miami, FL (K.N.); Department of Epidemiology, Robert Stempel College of Public Health, Florida International University, Miami (K.N.); Department of Medicine, Herbert Wertheim College of Medicine, Miami, FL (K.N.); Cardiovascular Division, Brigham and Women's Hospital, Boston, MA (R.B.); Los Angeles Biomedical Research Institute at Harbor-UCLA, Torrance, CA (M.J.B.); and Department of Preventive Medicine (P.G.) and Department of Medicine (P.G.), Northwestern University Feinberg School of Medicine, Chicago, IL.
Circ Cardiovasc Qual Outcomes. 2014 May;7(3):453-60. doi: 10.1161/CIRCOUTCOMES.113.000690. Epub 2014 May 6.
Aspirin for the primary prevention of coronary heart disease (CHD) is only recommended for individuals at high risk for CHD although the majority of CHD events occur in individuals who are at low to intermediate risk.
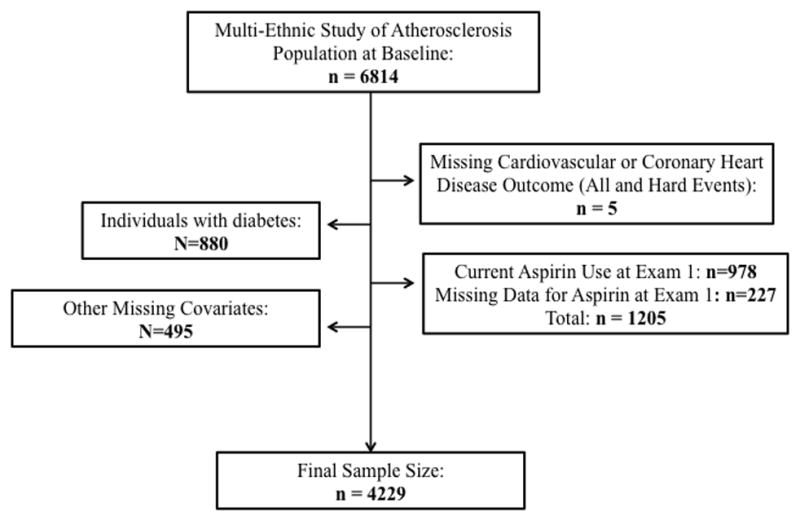
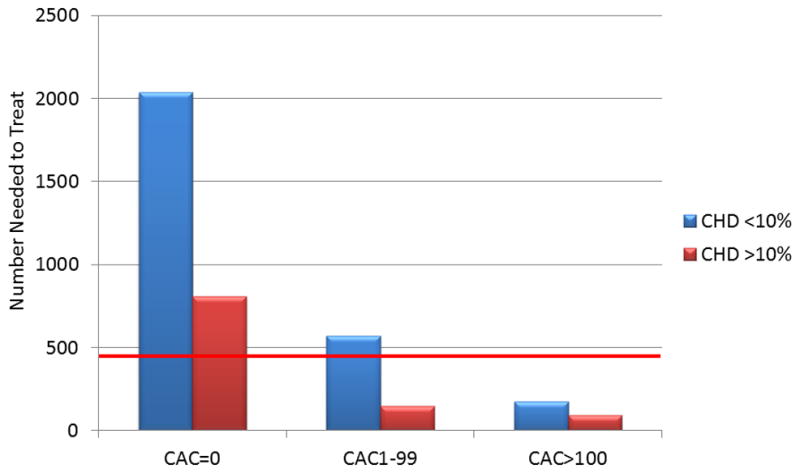
To estimate the potential of coronary artery calcium (CAC) scoring to guide aspirin use for primary prevention of CHD, we studied 4229 participants from the Multi-Ethnic Study of Atherosclerosis who were not on aspirin at baseline and were free of diabetes mellitus. Using data from median 7.6-year follow-up, 5-year number-needed-to-treat estimations were calculated by applying an 18% relative CHD reduction to the observed event rates. This was contrasted to 5-year number-needed-to-harm estimations based on the risk of major bleeding reported in an aspirin meta-analysis. Results were stratified by a 10% 10-year CHD Framingham Risk Score (FRS). Individuals with CAC≥100 had an estimated net benefit with aspirin regardless of their traditional risk status (estimated 5-year number needed to treat of 173 for individuals <10% FRS and 92 for individuals ≥10% FRS, estimated 5-year number needed to harm of 442 for a major bleed). Conversely, individuals with zero CAC had unfavorable estimations (estimated 5-year number needed to treat of 2036 for individuals <10% FRS and 808 for individuals ≥10% FRS, estimated 5-year number needed to harm of 442 for a major bleed). Sex-specific and age-stratified analyses showed similar results.
For the primary prevention of CHD, Multi-Ethnic Study of Atherosclerosis participants with CAC≥100 had favorable risk/benefit estimations for aspirin use while participants with zero CAC were estimated to receive net harm from aspirin.
阿司匹林用于冠心病(CHD)的一级预防仅推荐给冠心病高危个体,尽管大多数冠心病事件发生在低至中度风险的个体中。
为评估冠状动脉钙化(CAC)评分指导阿司匹林用于冠心病一级预防的潜力,我们研究了动脉粥样硬化多民族研究中的4229名参与者,这些参与者在基线时未服用阿司匹林且无糖尿病。利用中位7.6年随访数据,通过将冠心病相对降低18%应用于观察到的事件发生率来计算5年治疗所需人数估计值。这与基于阿司匹林荟萃分析中报告的大出血风险的5年伤害所需人数估计值形成对比。结果按10年冠心病弗雷明汉姆风险评分(FRS)为10%进行分层。CAC≥100的个体使用阿司匹林估计有净获益,无论其传统风险状态如何(FRS<10%的个体估计5年治疗所需人数为173,FRS≥10%的个体为92,大出血的估计5年伤害所需人数为442)。相反,CAC为零的个体估计结果不利(FRS<10%的个体估计5年治疗所需人数为2036,FRS≥10%的个体为808,大出血的估计5年伤害所需人数为442)。性别特异性和年龄分层分析显示了相似的结果。
对于冠心病的一级预防而言,动脉粥样硬化多民族研究中CAC≥100的参与者使用阿司匹林有良好的风险/获益估计,而CAC为零的参与者使用阿司匹林估计会受到净伤害。