Gini Rosa, Schuemie Martijn J, Francesconi Paolo, Lapi Francesco, Cricelli Iacopo, Pasqua Alessandro, Gallina Pietro, Donato Daniele, Brugaletta Salvatore, Donatini Andrea, Marini Alessandro, Cricelli Claudio, Damiani Gianfranco, Bellentani Mariadonata, van der Lei Johan, Sturkenboom Miriam C J M, Klazinga Niek S
Agenzia regionale di sanità della Toscana, Florence, Italy; Department of Medical Informatics, Erasmus Medical Center, Rotterdam, The Netherlands.
Department of Medical Informatics, Erasmus Medical Center, Rotterdam, The Netherlands.
PLoS One. 2014 May 9;9(5):e95419. doi: 10.1371/journal.pone.0095419. eCollection 2014.
Italy has a population of 60 million and a universal coverage single-payer healthcare system, which mandates collection of healthcare administrative data in a uniform fashion throughout the country. On the other hand, organization of the health system takes place at the regional level, and local initiatives generate natural experiments. This is happening in particular in primary care, due to the need to face the growing burden of chronic diseases. Health services research can compare and evaluate local initiatives on the basis of the common healthcare administrative data.However reliability of such data in this context needs to be assessed, especially when comparing different regions of the country. In this paper we investigated the validity of healthcare administrative databases to compute indicators of compliance with standards of care for diabetes, ischaemic heart disease (IHD) and heart failure (HF).
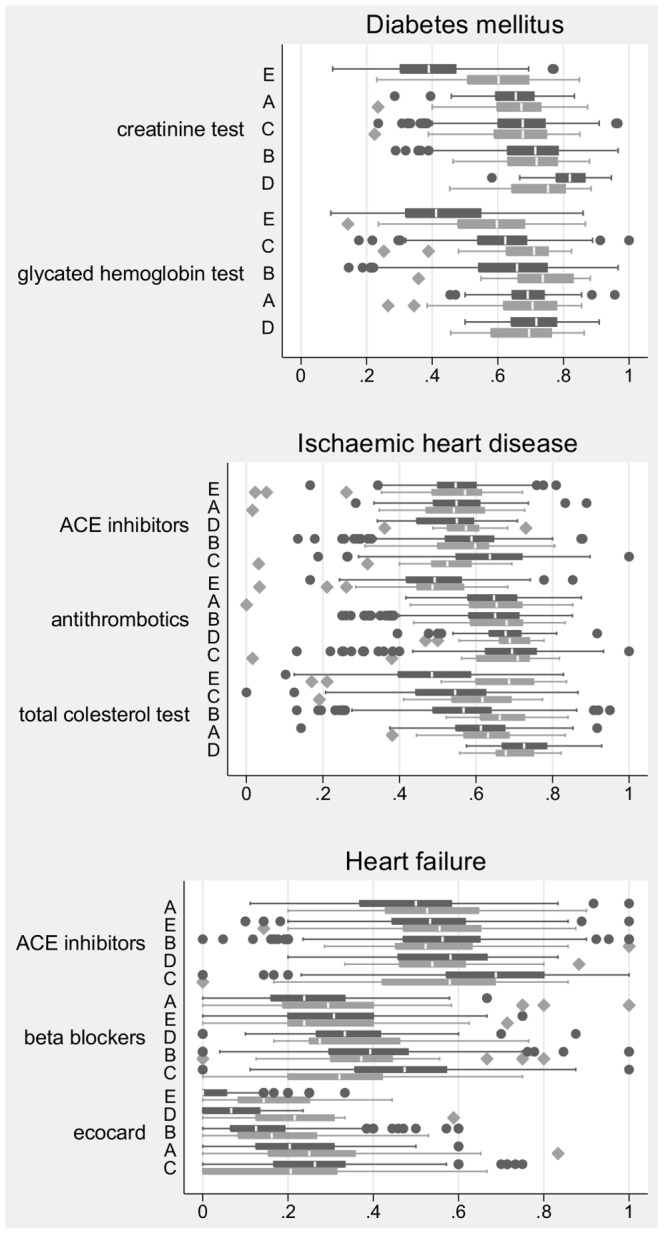
We compared indicators estimated from healthcare administrative data collected by Local Health Authorities in five Italian regions with corresponding estimates from clinical data collected by General Practitioners (GPs). Four indicators of diagnostic follow-up (two for diabetes, one for IHD and one for HF) and four indicators of appropriate therapy (two each for IHD and HF) were considered.
Agreement between the two data sources was very good, except for indicators of laboratory diagnostic follow-up in one region and for the indicator of bioimaging diagnostic follow-up in all regions, where measurement with administrative data underestimated quality.
According to evidence presented in this study, estimating compliance with standards of care for diabetes, ischaemic heart disease and heart failure from healthcare databases is likely to produce reliable results, even though completeness of data on diagnostic procedures should be assessed first. Performing studies comparing regions using such indicators as outcomes is a promising development with potential to improve quality governance in the Italian healthcare system.
意大利有6000万人口,实行全民覆盖的单一支付者医疗保健系统,该系统要求在全国以统一方式收集医疗保健管理数据。另一方面,卫生系统在地区层面组织,地方举措会产生自然实验。这尤其发生在初级保健领域,因为需要应对慢性病日益加重的负担。卫生服务研究可以根据通用的医疗保健管理数据比较和评估地方举措。然而,在此背景下此类数据的可靠性需要评估,尤其是在比较该国不同地区时。在本文中,我们调查了医疗保健管理数据库计算糖尿病、缺血性心脏病(IHD)和心力衰竭(HF)护理标准合规指标的有效性。
我们将意大利五个地区地方卫生当局收集的医疗保健管理数据估算的指标与全科医生(GPs)收集的临床数据的相应估算值进行了比较。考虑了四个诊断随访指标(糖尿病两个、IHD一个、HF一个)和四个适当治疗指标(IHD和HF各两个)。
除了一个地区的实验室诊断随访指标以及所有地区的生物成像诊断随访指标外,两个数据源之间的一致性非常好,在这些指标中,管理数据测量低估了质量。
根据本研究提供的证据,从医疗保健数据库估算糖尿病、缺血性心脏病和心力衰竭的护理标准合规情况可能会得出可靠结果,尽管应首先评估诊断程序数据的完整性。使用此类指标作为结果比较各地区的研究是一个有前景的发展方向,有可能改善意大利医疗保健系统的质量治理。