Department of Clinical and Experimental Medicine, Unit of Pharmacology and Pharmacovigilance, University of Pisa, Pisa, Italy.
Unit of Rheumatology, University Hospital of Pisa, Pisa, Italy.
Sci Rep. 2021 Oct 13;11(1):20314. doi: 10.1038/s41598-021-98321-0.
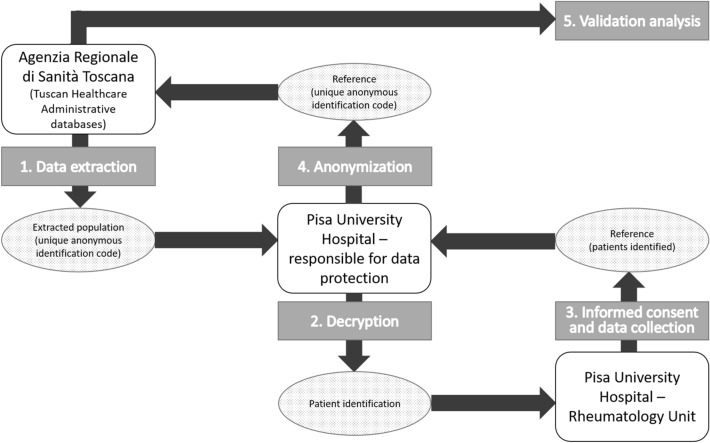
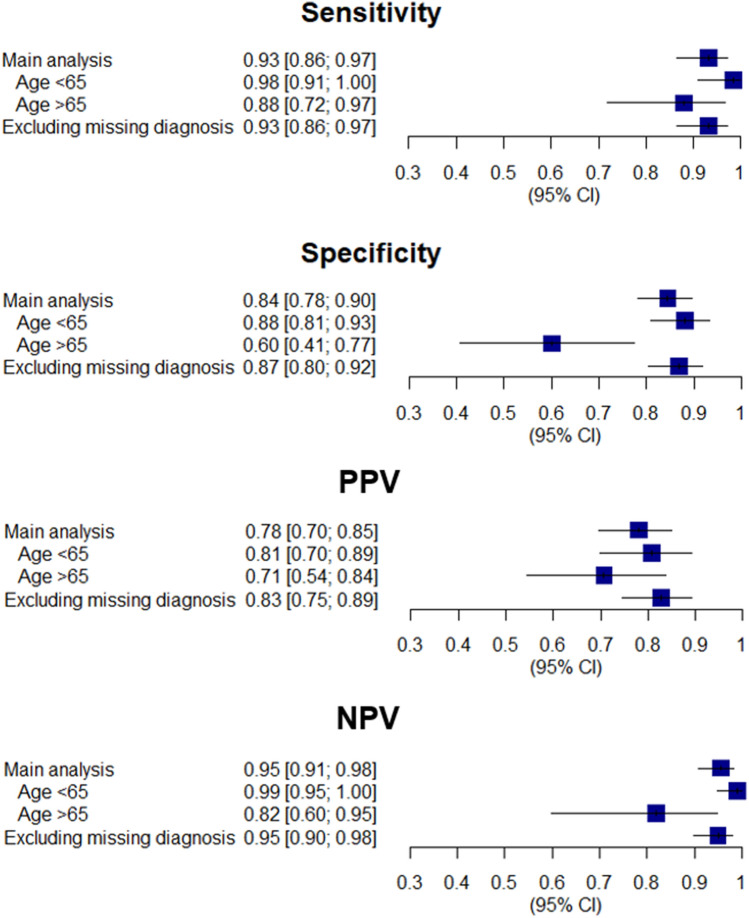
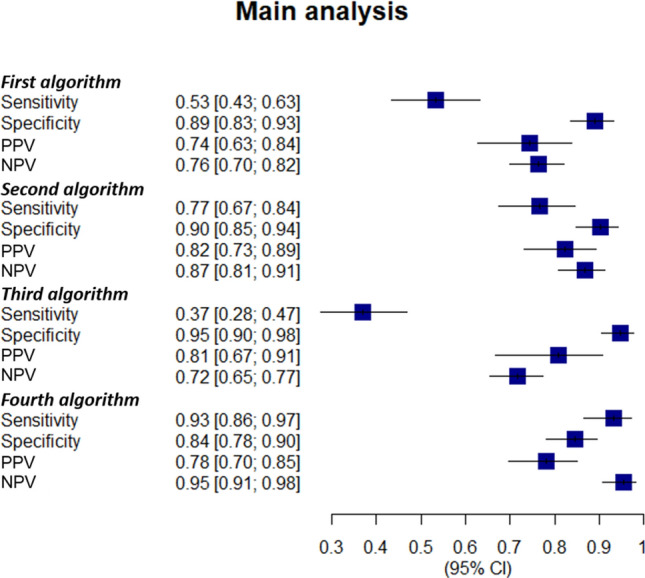
Validation of algorithms for selecting patients from healthcare administrative databases (HAD) is recommended. This PATHFINDER study section is aimed at testing algorithms to select rheumatoid arthritis (RA) patients from Tuscan HAD (THAD) and assessing RA diagnosis time interval between the medical chart date and that of THAD. A population was extracted from THAD. The information of the medical charts at the Rheumatology Unit of Pisa University Hospital represented the reference. We included first ever users of biologic disease modifying anti-rheumatic drugs (bDMARDs) between 2014 and 2016 (index date) with at least a specialist visit at the Rheumatology Unit of the Pisa University Hospital recorded from 2013 to the index date. Out of these, we tested four index tests (algorithms): (1) RA according to hospital discharge records or emergency department admissions (ICD-9 code, 714*); (2) RA according to exemption code from co-payment (006); (3) RA according to hospital discharge records or emergency department admissions AND RA according to exemption code from co-payment; (4) RA according to hospital discharge records or emergency department admissions OR RA according to exemption code from co-payment. We estimated sensitivity, specificity, positive and negative predicted values (PPV and NPV) with 95% confidence interval (95% CI) and the RA diagnosis median time interval (interquartile range, IQR). Two sensitivity analyses were performed. Among 277 reference patients, 103 had RA. The fourth algorithm identified 96 true RA patients, PPV 0.78 (95% CI 0.70-0.85), sensitivity 0.93 (95% CI 0.86-0.97), specificity 0.84 (95% CI 0.78-0.90), and NPV 0.95 (95% CI 0.91-0.98). The sensitivity analyses confirmed performance. The time measured between the actual RA diagnosis date recorded in medical charts and that assumed in THAD was 2.2 years (IQR 0.5-8.4). In conclusion, this validation showed the fourth algorithm as the best. The time interval elapsed between the actual RA diagnosis date in medical charts and that extrapolated from THAD has to be considered in the design of future studies.
验证从医疗保健管理数据库(HAD)中选择患者的算法是推荐的。本 PATHFINDER 研究部分旨在测试从托斯卡纳 HAD(THAD)中选择类风湿关节炎(RA)患者的算法,并评估医疗图表日期和 THAD 之间的 RA 诊断时间间隔。从 THAD 中提取了一个人群。比萨大学医院风湿病科的医疗图表信息代表了参考。我们纳入了 2014 年至 2016 年(索引日期)首次使用生物疾病修正抗风湿药物(bDMARDs)的患者,且至少有一次在比萨大学医院风湿病科的专家就诊记录,记录时间从 2013 年到索引日期。在这些患者中,我们测试了四种索引测试(算法):(1)根据医院出院记录或急诊入院的 RA(ICD-9 代码,714*);(2)根据共付额豁免代码的 RA(006);(3)根据医院出院记录或急诊入院的 RA 和根据共付额豁免代码的 RA;(4)根据医院出院记录或急诊入院的 RA 或根据共付额豁免代码的 RA。我们使用 95%置信区间(95%CI)和 RA 诊断中位时间间隔(四分位间距,IQR)估计了敏感性、特异性、阳性和阴性预测值(PPV 和 NPV)。进行了两次敏感性分析。在 277 名参考患者中,有 103 名患有 RA。第四种算法确定了 96 名真正的 RA 患者,PPV 为 0.78(95%CI 0.70-0.85),敏感性为 0.93(95%CI 0.86-0.97),特异性为 0.84(95%CI 0.78-0.90),NPV 为 0.95(95%CI 0.91-0.98)。敏感性分析证实了性能。在医疗图表中记录的实际 RA 诊断日期和 THAD 中假设的日期之间测量的时间为 2.2 年(IQR 0.5-8.4)。总之,本验证表明第四种算法是最好的。在设计未来的研究时,必须考虑从医疗图表中实际 RA 诊断日期和从 THAD 中推断出的日期之间的时间间隔。