Biological Sciences Division, Pathology, The University of Chicago, 929 E. 57th Street, GCIS W-423, Chicago, IL 60637, USA.
Department of Pathology and Department of Medicine, Section of Hematology/Oncology, The University of Chicago, 5841 S. Maryland Ave., MC2115, Chicago, IL 60637, USA.
J Immunother Cancer. 2013 Sep 23;1:16. doi: 10.1186/2051-1426-1-16. eCollection 2013.
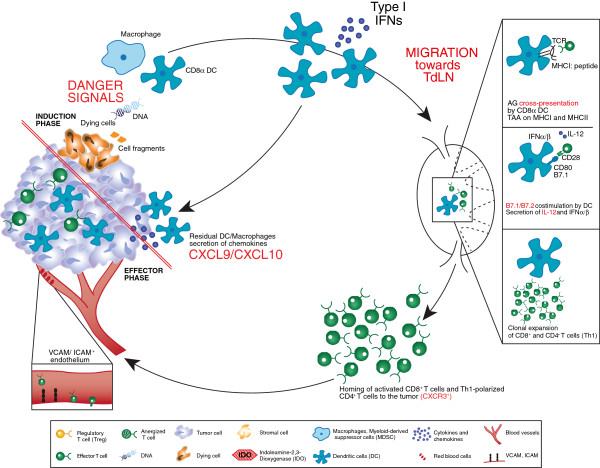
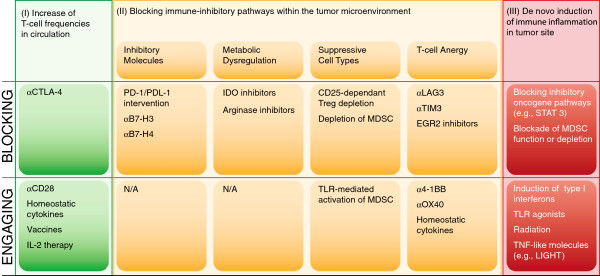
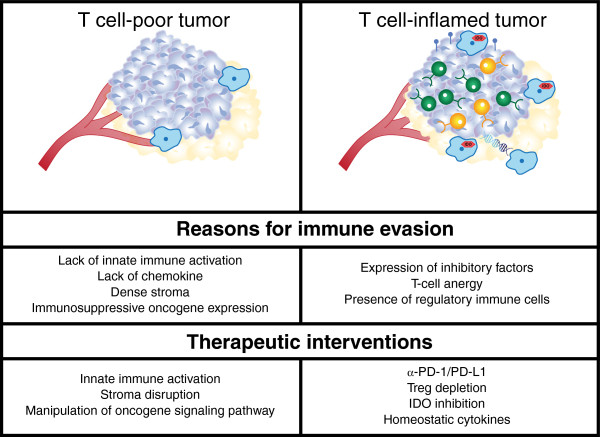
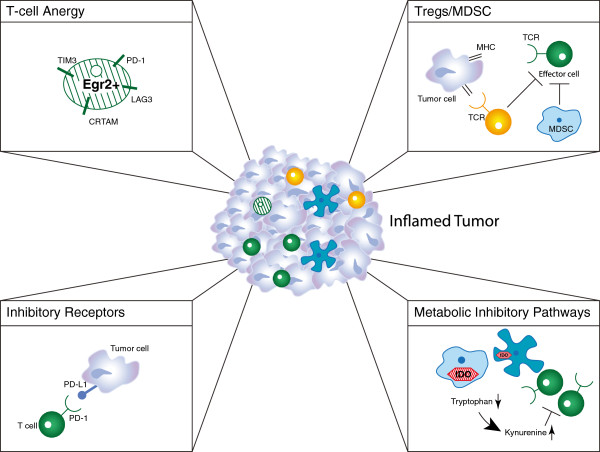
An effective anti-tumor immune response requires the coordinated action of the innate and adaptive phases of the immune system. Critical processes include the activation of dendritic cells to present antigens, produce cytokines including type I interferons, and express multiple costimulatory ligands; induction of a productive T cell response within lymph nodes; migration of activated T cells to the tumor microenvironment in response to chemokines and homing receptor expression; and having effector T cells gain access to antigen-expressing tumor cells and maintain sufficient functionality to destroy them. However, tumors can become adept at escaping the immune response, developing multiple mechanisms to disrupt key processes. In general, tumors can be assigned into two different, major groups depending on whether the tumor there is an 'inflamed' or 'non-inflamed' tumor microenvironment. Improvements in our understanding of the interactions between the immune system and cancer have resulted in the development of various strategies to improve the immune-mediated control of tumors in both sub-groups. Categories of major immunotherapeutic intervention include methods to increase the frequency of tumor antigen-specific effector T cells in the circulation, strategies to block or uncouple a range of immune suppressive mechanisms within the tumor microenvironment, and tactics to induce de novo immune inflammation within the tumor microenvironment. The latter may be particularly important for eliciting immune recognition of non-inflamed tumor phenotypes. The premise put forth in this review is that synergistic therapeutic effects in vivo may be derived from combination therapies taken from distinct "bins" based on these mechanisms of action. Early data in both preclinical and some clinical studies provide support for this model. We also suggest that optimal application of these combinations may be aided by appropriate patient selection based on predictive biomarkers.
有效的抗肿瘤免疫反应需要免疫系统的先天和适应性阶段的协调作用。关键过程包括激活树突状细胞以呈递抗原、产生包括 I 型干扰素在内的细胞因子,并表达多种共刺激配体;在淋巴结中诱导有效的 T 细胞反应;趋化因子和归巢受体表达后,激活的 T 细胞迁移到肿瘤微环境中;效应 T 细胞获得表达抗原的肿瘤细胞,并保持足够的功能来破坏它们。然而,肿瘤可以变得擅长逃避免疫反应,发展多种机制来破坏关键过程。一般来说,肿瘤可以根据肿瘤微环境是“炎症”还是“非炎症”分为两个不同的主要组。我们对免疫系统与癌症之间相互作用的理解的提高导致了各种策略的发展,以改善这两个亚组中肿瘤的免疫介导控制。主要免疫治疗干预的类别包括增加循环中肿瘤抗原特异性效应 T 细胞频率的方法、阻断或分离肿瘤微环境中一系列免疫抑制机制的策略,以及诱导肿瘤微环境中新生免疫炎症的策略。后者对于引发对非炎症性肿瘤表型的免疫识别可能尤为重要。这篇综述提出的前提是,基于这些作用机制,来自不同“框”的联合治疗可能会在体内产生协同治疗效果。临床前和一些临床研究的早期数据为这一模型提供了支持。我们还建议,基于预测性生物标志物进行适当的患者选择,可能有助于这些组合的最佳应用。