Flint Alexander C, Cullen Sean P, Rao Vivek A, Faigeles Bonnie S, Pereira Vitor M, Levy Elad I, Jovin Tudor G, Liebeskind David S, Nogueira Raul G, Jahan Reza, Saver Jeffrey L
Department of Neuroscience, Kaiser Permanente, Redwood City, CA, USA.
Int J Stroke. 2014 Aug;9(6):698-704. doi: 10.1111/ijs.12292. Epub 2014 May 20.
The Totaled Health Risks in Vascular Events (THRIVE) score strongly predicts clinical outcome, mortality, and risk of thrombolytic haemorrhage in ischemic stroke patients, and performs similarly well in patients receiving intravenous tissue plasminogen activator, endovascular stroke treatment, or no acute treatment. It is not known if the THRIVE score predicts outcomes with the Solitaire endovascular stroke treatment device.
To validate the relationship between the THRIVE score and outcomes after treatment with the Solitaire endovascular stroke treatment device.
The study conducted a retrospective analysis of the prospective SWIFT and STAR trials to examine the relationship between THRIVE and outcomes after treatment with the Solitaire device. We examined the relationship between THRIVE and clinical outcomes (good outcome or death at 90 days) among patients in SWIFT and STAR. Receiver-operator characteristics curve analysis was used to compare THRIVE score performance with other stroke prediction scores. Multivariable modeling was used to confirm the independence of the THRIVE score from procedure-specific predictors (successful recanalization or device used) and other predictors of functional outcome.
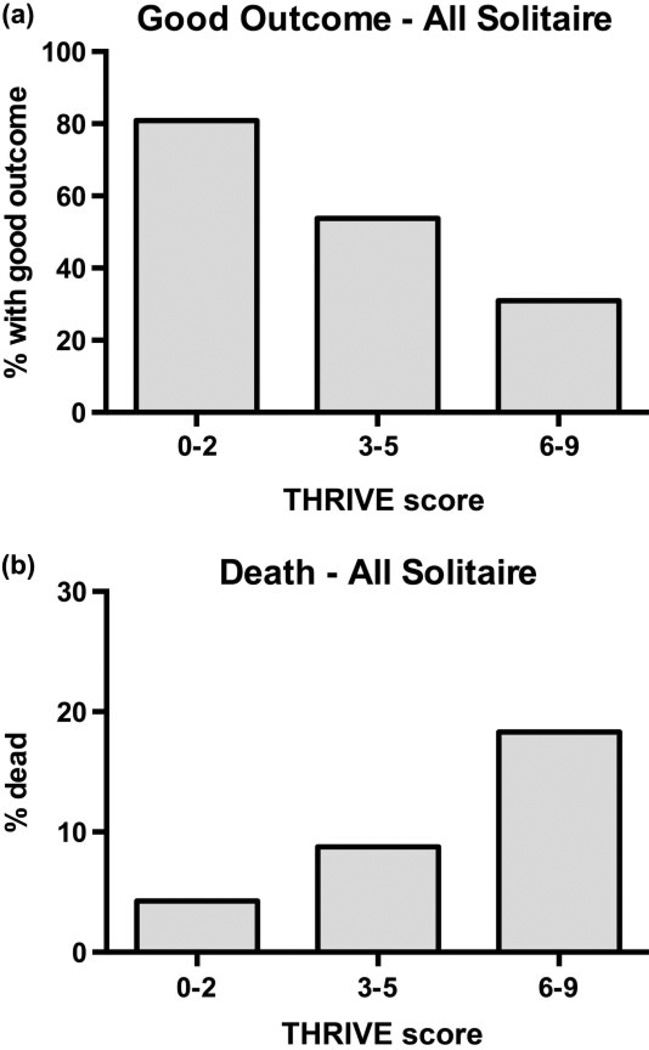
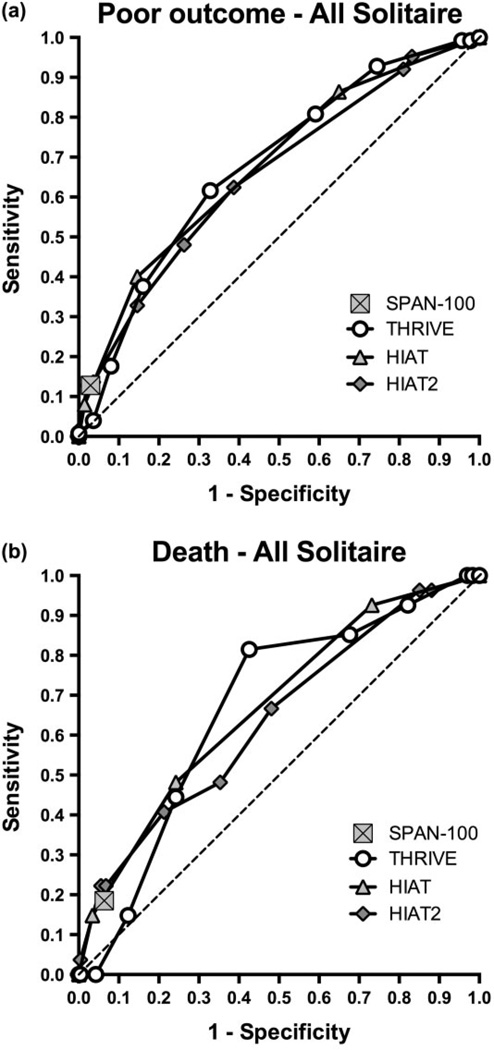
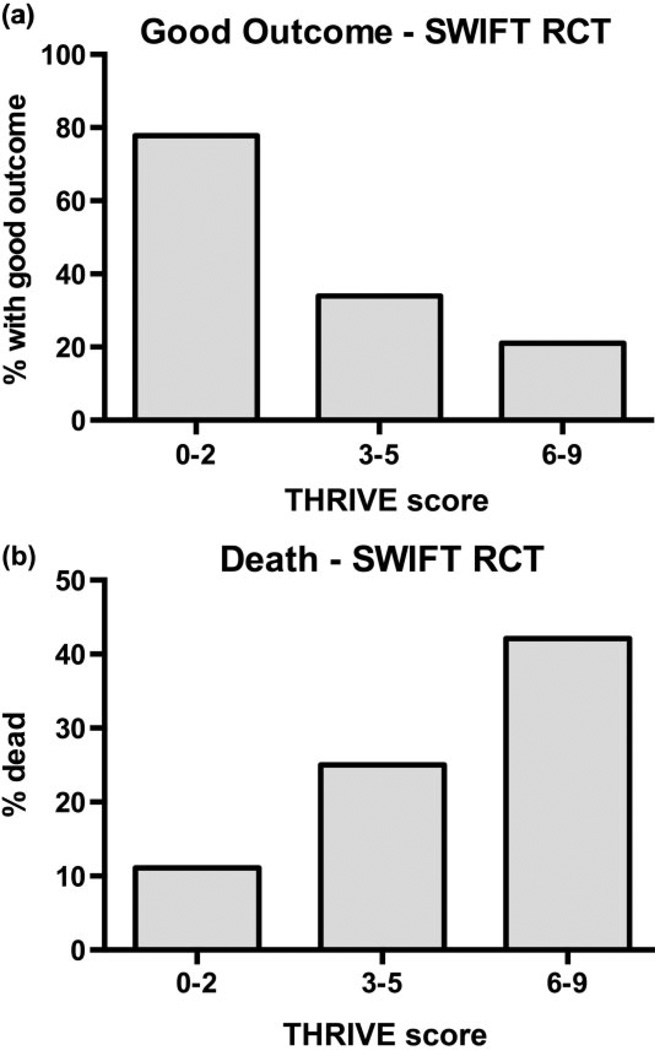
The THRIVE score strongly predicts good outcome and death among patients treated with the Solitaire device in SWIFT and STAR (Mantel-Haenszel chi-square test for trend P < 0·001 for good outcome, P = 0·01 for death). In receiver-operator characteristics (ROC) curve comparisons, totaled health risks in vascular events score is superior to Stroke Prognostication using Age and NIH Stroke Scale score-100 (P < 0·001) and performed similarly to Houston Intra-Arterial Therapy score (HIAT) (P = 0·98) and HIAT-2 (P = 0·54). In multivariable models, THRIVE's prediction of good outcome is not altered after controlling for recanalization or after controlling for device used. The THRIVE score remains a strong independent predictor after controlling for the above predictors together with time to procedure, rate of symptomatic haemorrhage, and use of general anesthesia. Of note, use of general anesthesia was not an independent predictor of outcome in SWIFT + STAR after controlling for totaled health risks in vascular events and other factors.
The THRIVE score strongly predicts clinical outcome and mortality in patients treated with the Solitaire device in the SWIFT and STAR trials. The lack of interaction between THRIVE and procedure-specific elements such as vessel recanalization or device choice makes the THRIVE score a reasonable candidate for use as a patient selection criterion in stroke clinical trials.
血管事件总体健康风险(THRIVE)评分能有力预测缺血性中风患者的临床结局、死亡率和溶栓性出血风险,在接受静脉注射组织纤溶酶原激活剂、血管内中风治疗或未接受急性治疗的患者中表现同样出色。目前尚不清楚THRIVE评分能否预测使用Solitaire血管内中风治疗装置后的结局。
验证THRIVE评分与使用Solitaire血管内中风治疗装置治疗后的结局之间的关系。
该研究对前瞻性SWIFT和STAR试验进行回顾性分析,以研究THRIVE与使用Solitaire装置治疗后的结局之间的关系。我们研究了SWIFT和STAR试验中患者的THRIVE与临床结局(90天时良好结局或死亡)之间的关系。采用受试者工作特征曲线分析,将THRIVE评分表现与其他中风预测评分进行比较。使用多变量模型来确认THRIVE评分独立于特定手术预测因素(成功再通或使用的装置)以及功能结局的其他预测因素。
在SWIFT和STAR试验中,THRIVE评分能有力预测使用Solitaire装置治疗的患者出现良好结局和死亡情况(对于良好结局,趋势的Mantel-Haenszel卡方检验P<0.001;对于死亡,P = 0.01)。在受试者工作特征(ROC)曲线比较中,血管事件总体健康风险评分优于使用年龄和美国国立卫生研究院中风量表评分-100进行的中风预后评估(P<0.001),与休斯顿动脉内治疗评分(HIAT)(P = 0.98)和HIAT-2(P = 0.54)表现相似。在多变量模型中,在控制再通或控制使用的装置后,THRIVE对良好结局的预测不变。在控制上述预测因素以及手术时间、症状性出血发生率和全身麻醉使用情况后,THRIVE评分仍然是一个强有力的独立预测因素。值得注意的是在控制血管事件总体健康风险和其他因素后,全身麻醉的使用在SWIFT + STAR试验中并非结局的独立预测因素。
在SWIFT和STAR试验中,THRIVE评分能有力预测使用Solitaire装置治疗的患者的临床结局和死亡率。THRIVE与诸如血管再通或装置选择等特定手术因素之间缺乏相互作用,这使得THRIVE评分成为中风临床试验中用作患者选择标准的合理候选因素。