Hawley Sarah T, Jagsi Reshma, Morrow Monica, Janz Nancy K, Hamilton Ann, Graff John J, Katz Steven J
Medical School, University of Michigan, Ann Arbor1VA Ann Arbor Healthcare System, Ann Arbor, Michigan3School of Public Health, University of Michigan, Ann Arbor.
Medical School, University of Michigan, Ann Arbor.
JAMA Surg. 2014 Jun;149(6):582-9. doi: 10.1001/jamasurg.2013.5689.
The growing rate of contralateral prophylactic mastectomy (CPM) among women diagnosed as having breast cancer has raised concerns about potential for overtreatment. Yet, there are few large survey studies of factors that affect women's decisions for this surgical treatment option.
To determine factors associated with the use of CPM in a population-based sample of patients with breast cancer.
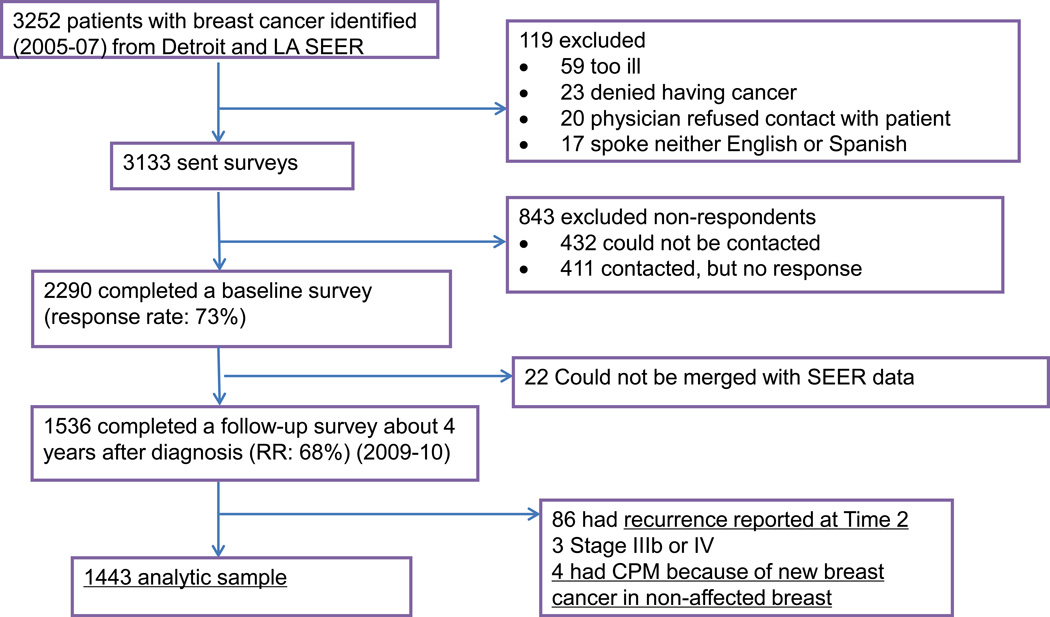
DESIGN, SETTING, AND PARTICIPANTS: A longitudinal survey of 2290 women newly diagnosed as having breast cancer who reported to the Detroit and Los Angeles Surveillance, Epidemiology, and End Results registries from June 1, 2005, to February 1, 2007, and again 4 years later (June 2009 to February 2010) merged with Surveillance, Epidemiology, and End Results registry data (n = 1536). Multinomial logistic regression was used to evaluate factors associated with type of surgery. Primary independent variables included clinical indications for CPM (genetic mutation and/or strong family history), diagnostic magnetic resonance imaging, and patient extent of worry about recurrence at the time of treatment decision making.
Type of surgery received from patient self-report, categorized as CPM, unilateral mastectomy, or breast conservation surgery.
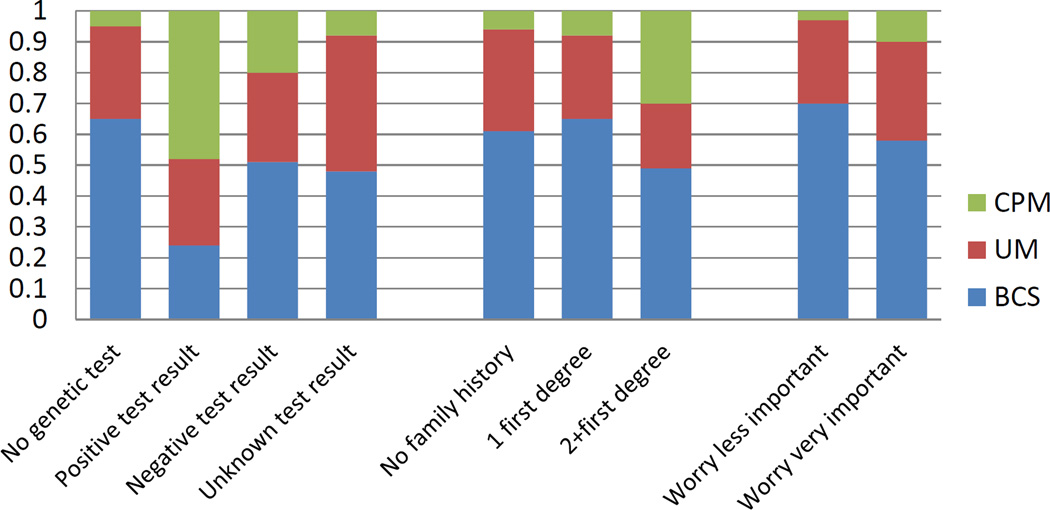
Of the 1447 women in the analytic sample, 18.9% strongly considered CPM and 7.6% received it. Of those who strongly considered CPM, 32.2% received CPM, while 45.8% received unilateral mastectomy and 22.8% received breast conservation surgery (BCS). The majority of patients (68.9%) who received CPM had no major genetic or familial risk factors for contralateral disease. Multivariate regression showed that receipt of CPM (vs either unilateral mastectomy or breast conservation surgery) was significantly associated with genetic testing (positive or negative) (vs UM, relative risk ratio [RRR]: 10.48; 95% CI, 3.61-3.48 and vs BCS, RRR: 19.10; 95% CI, 5.67-56.41; P < .001), a strong family history of breast or ovarian cancer (vs UM, RRR: 5.19; 95% CI, 2.34-11.56 and vs BCS, RRR: 4.24; 95% CI, 1.80-9.88; P = .001), receipt of magnetic resonance imaging (vs UM RRR: 2.07; 95% CI, 1.21-3.52 and vs BCS, RRR: 2.14; 95% CI, 1.28-3.58; P = .001), higher education (vs UM, RRR: 5.04; 95% CI, 2.37-10.71 and vs BCS, RRR: 4.38; 95% CI, 2.07-9.29; P < .001), and greater worry about recurrence (vs UM, RRR: 2.81; 95% CI, 1.14-6.88 and vs BCS, RRR: 4.24; 95% CI, 1.80-9.98; P = .001).
Many women considered CPM and a substantial number received it, although few had a clinically significant risk of contralateral breast cancer. Receipt of magnetic resonance imaging at diagnosis contributed to receipt of CPM. Worry about recurrence appeared to drive decisions for CPM although the procedure has not been shown to reduce recurrence risk. More research is needed about the underlying factors driving the use of CPM.
被诊断患有乳腺癌的女性中,对侧预防性乳房切除术(CPM)的实施率不断上升,引发了对过度治疗可能性的担忧。然而,关于影响女性选择这种手术治疗方案的因素,大型调查研究较少。
确定在以人群为基础的乳腺癌患者样本中,与CPM使用相关的因素。
设计、地点和参与者:对2290名新诊断为乳腺癌的女性进行纵向调查,这些女性于2005年6月1日至2007年2月1日向底特律和洛杉矶监测、流行病学和最终结果登记处报告情况,并在4年后(2009年6月至2010年2月)再次报告,数据与监测、流行病学和最终结果登记处数据合并(n = 1536)。采用多项逻辑回归评估与手术类型相关的因素。主要自变量包括CPM的临床指征(基因突变和/或家族病史强烈)、诊断性磁共振成像以及治疗决策时患者对复发的担忧程度。
患者自我报告的手术类型,分为CPM、单侧乳房切除术或保乳手术。
在分析样本的l447名女性中,18.9%强烈考虑CPM,7.6%接受了该手术。在强烈考虑CPM的女性中,32.2%接受了CPM,而45.8%接受了单侧乳房切除术,22.8%接受了保乳手术(BCS)。接受CPM的大多数患者(68.9%)没有对侧疾病的主要遗传或家族风险因素。多变量回归显示,接受CPM(与单侧乳房切除术或保乳手术相比)与基因检测(阳性或阴性)显著相关(与单侧乳房切除术相比,相对风险比[RRR]:10.48;95%置信区间,3.61 - 3.48;与保乳手术相比,RRR:19.10;95%置信区间,5.67 - 56.41;P <.001)、乳腺癌或卵巢癌家族病史强烈(与单侧乳房切除术相比,RRR:5.19;95%置信区间,2.34 - 1l.56;与保乳手术相比,RRR:4.24;95%置信区间,1.80 - l9.88;P =.001)、接受磁共振成像(与单侧乳房切除术相比,RRR:2.07;95%置信区间,1.21 - 3.52;与保乳手术相比,RRR:2.14;95%置信区间,1.28 - 3.58;P =.001)、高等教育程度(与单侧乳房切除术相比,RRR:5.04;95%置信区间,2.37 - 10.71;与保乳手术相比,RRR:4.38;95%置信区间,2.07 - 9.l9;P <.001)以及对复发的更大担忧(与单侧乳房切除术相比,RRR:2.81;95%置信区间,1.14 - 6.88;与保乳手术相比,RRR:4.24;95%置信区间,1.80 - 9.98;P =.001)相关。
许多女性考虑了CPM,相当一部分女性接受了该手术,尽管很少有人有对侧乳腺癌的临床显著风险。诊断时接受磁共振成像有助于CPM的实施。对复发的担忧似乎推动了CPM的决策,尽管该手术尚未被证明能降低复发风险。需要对推动CPM使用的潜在因素进行更多研究。