Medical University of South Carolina, Charleston.
Indiana University, Indianapolis.
JAMA. 2014 May;311(20):2101-9. doi: 10.1001/jama.2014.5220.
Abdominal pain after cholecystectomy is common and may be attributed to sphincter of Oddi dysfunction. Management often involves endoscopic retrograde cholangiopancreatography (ERCP) with manometry and sphincterotomy.
To determine whether endoscopic sphincterotomy reduces pain and whether sphincter manometric pressure is predictive of pain relief.
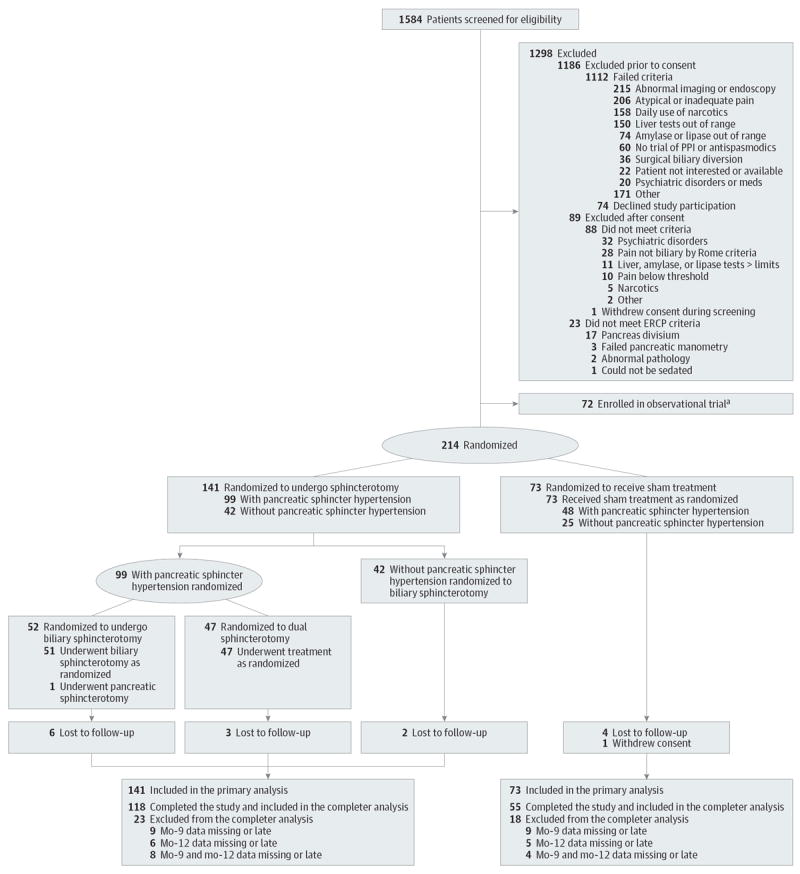
DESIGN, SETTING, AND PATIENTS: Multicenter, sham-controlled, randomized trial involving 214 patients with pain after cholecystectomy without significant abnormalities on imaging or laboratory studies, and no prior sphincter treatment or pancreatitis randomly assigned (August 6, 2008-March 23, 2012) to undergo sphincterotomy or sham therapy at 7 referral medical centers. One-year follow-up was blinded. The final follow-up visit was March 21, 2013.
After ERCP, patients were randomized 2:1 to sphincterotomy (n = 141) or sham (n = 73) irrespective of manometry findings. Those randomized to sphincterotomy with elevated pancreatic sphincter pressures were randomized again (1:1) to biliary or to both biliary and pancreatic sphincterotomies. Seventy-two were entered into an observational study with conventional ERCP managemeny.
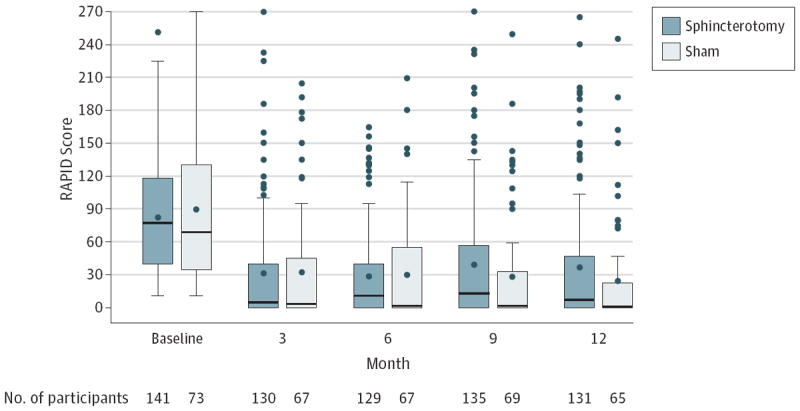
Success of treatment was defined as less than 6 days of disability due to pain in the prior 90 days both at months 9 and 12 after randomization, with no narcotic use and no further sphincter intervention.
Twenty-seven patients (37%; 95% CI, 25.9%-48.1%) in the sham treatment group vs 32 (23%; 95% CI, 15.8%-29.6%) in the sphincterotomy group experienced successful treatment (adjusted risk difference, -15.6%; 95% CI, -28.0% to -3.3%; P = .01). Of the patients with pancreatic sphincter hypertension, 14 (30%; 95% CI, 16.7%-42.9%) who underwent dual sphincterotomy and 10 (20%; 95% CI, 8.7%-30.5%) who underwent biliary sphincterotomy alone experienced successful treatment. Thirty-seven treated patients (26%; 95% CI,19%-34%) and 25 patients (34%; 95% CI, 23%-45%) in the sham group underwent repeat ERCP interventions (P = .22). Manometry results were not associated with the outcome. No clinical subgroups appeared to benefit from sphincterotomy more than others. Pancreatitis occurred in 15 patients (11%) after primary sphincterotomies and in 11 patients (15%) in the sham group. Of the nonrandomized patients in the observational study group, 5 (24%; 95% CI, 6%-42%) who underwent biliary sphincterotomy, 12 (31%; 95% CI, 16%-45%) who underwent dual sphincterotomy, and 2 (17%; 95% CI, 0%-38%) who did not undergo sphincterotomy had successful treatment.
In patients with abdominal pain after cholecystectomy undergoing ERCP with manometry, sphincterotomy vs sham did not reduce disability due to pain. These findings do not support ERCP and sphincterotomy for these patients.
clinicaltrials.gov Identifier: NCT00688662.
胆囊切除术后出现腹痛很常见,可能归因于Oddi 括约肌功能障碍。治疗通常涉及内镜逆行胰胆管造影(ERCP)并进行测压和括约肌切开术。
确定内镜括约肌切开术是否能减轻疼痛,以及括约肌测压是否能预测疼痛缓解。
设计、地点和患者:多中心、假对照、随机试验,涉及 214 例胆囊切除术后出现疼痛但影像学或实验室检查无明显异常、无先前括约肌治疗或胰腺炎的患者,在 7 家转诊医疗中心随机分配(2008 年 8 月 6 日至 2012 年 3 月 23 日)行括约肌切开术或假治疗。对 1 年的随访进行了盲法。最终随访时间为 2013 年 3 月 21 日。
ERCP 后,根据测压结果,患者被随机分为括约肌切开术组(n=141)或假治疗组(n=73),无论测压结果如何。那些括约肌切开术组中胰腺括约肌压力升高的患者再次随机(1:1)分为胆管或胆管和胰腺括约肌切开术组。72 例患者进入常规 ERCP 管理的观察性研究。
治疗成功定义为随机分组后 90 天内前 90 天因疼痛导致的残疾天数少于 6 天,无阿片类药物使用,且无需进一步行括约肌干预。
假治疗组中 27 例(37%;95%CI,25.9%-48.1%)和括约肌切开术组中 32 例(23%;95%CI,15.8%-29.6%)患者的治疗成功(调整后的风险差异,-15.6%;95%CI,-28.0%至-3.3%;P=0.01)。在胰腺括约肌高压患者中,行双括约肌切开术的 14 例(30%;95%CI,16.7%-42.9%)和单独行胆管括约肌切开术的 10 例(20%;95%CI,8.7%-30.5%)患者的治疗成功。37 例治疗患者(26%;95%CI,19%-34%)和假治疗组的 25 例患者(34%;95%CI,23%-45%)行重复 ERCP 干预(P=0.22)。测压结果与结果无关。没有任何临床亚组似乎比其他亚组更受益于括约肌切开术。原发性括约肌切开术后 15 例(11%)和假治疗组中 11 例(15%)患者发生胰腺炎。在观察性研究组中未随机分组的患者中,行胆管括约肌切开术的 5 例(24%;95%CI,6%-42%)、行双括约肌切开术的 12 例(31%;95%CI,16%-45%)和未行括约肌切开术的 2 例(17%;95%CI,0%-38%)患者的治疗成功。
在接受 ERCP 测压的胆囊切除术后腹痛患者中,括约肌切开术与假治疗相比并未减少疼痛导致的残疾。这些发现不支持对这些患者进行 ERCP 和括约肌切开术。
clinicaltrials.gov 标识符:NCT00688662。