Zeng Shuxiong, Zhang Zhensheng, Yu Xiaowen, Song Ruixiang, Wei Rongchao, Zhao Junjie, Wang Linhui, Hou Jianguo, Sun Yinghao, Xu Chuanliang
From the Department of Urology, Changhai Hospital, Second Military Medical University, Shanghai, P. R. China.
From the Department of Geriatrics, Changhai Hospital, Second Military Medical University, Shanghai, P. R. China.
PLoS One. 2014 Jun 5;9(6):e98950. doi: 10.1371/journal.pone.0098950. eCollection 2014.
To explore the morbidity, mortality and oncological results of laparoscopic radical cystectomy (LRC) in the elderly patients over 75-year-old in contrast with open radical cystectomy (ORC).
We analyzed 46 radical cystectomies from January 2009 to December 2013 in patients over 75-year-old in our institute, 21 patients in the LRC group and 25 in the ORC group. Demographic parameters, operative variables and perioperative outcome were retrospectively collected and analyzed between the two groups. Perioperative morbidity and mortality were categorized as early (within 90 days after surgery) or late (more than 90 days) according to the time of occurrence.
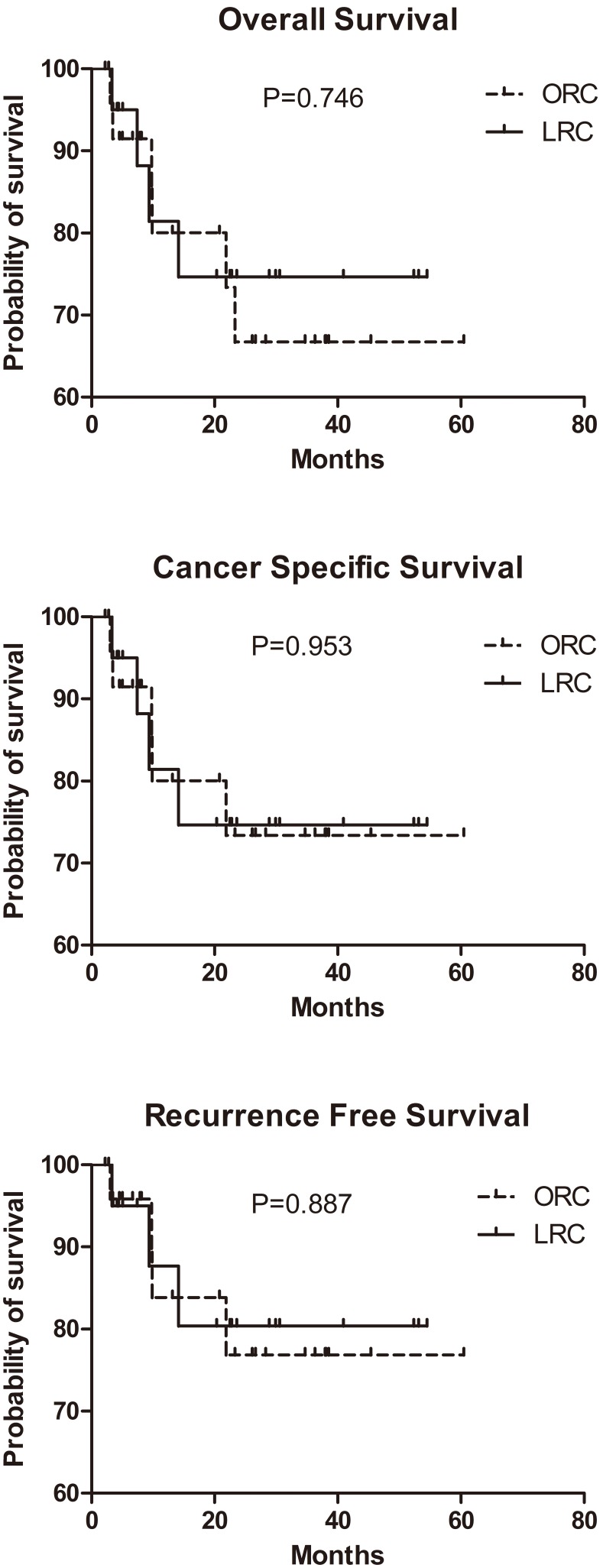
Patients in both groups had comparable preoperative characteristics. A significant longer operative time (418 vs. 337 min, p = 0.018) and less estimated blood loss (400 vs. 500 ml p = 0.038) were observed in LRC group compared with ORC group. Infection and ileus were the most common early complications after surgery. Patients underwent ORC suffered from significantly more postoperative ileus (28.0% vs. 4.8%, P = 0.038) and infection (40% vs. 9.5%, P = 0.019) than LRC group within 90 days after surgery. The mortality rate was 4.7% (1/21) and 4% (1/25) for LRC group and ORC group respectively. At a median follow-up of 21 months (range 2-61 months), the Kaplan-Meier survival curves and log-rank analysis demonstrate that there were no significant differences between the LRC and ORC groups in the 3-year overall, cancer-specific, or recurrence-free survival rates.
It is suggested that LRC should be recommended as the primary intervention to treat muscle invasive or high risk non-muscle invasive bladder cancer in elderly patients with a relative long life expectancy.
探讨75岁以上老年患者腹腔镜根治性膀胱切除术(LRC)与开放性根治性膀胱切除术(ORC)的发病率、死亡率及肿瘤学结果。
我们分析了2009年1月至2013年12月在我院接受根治性膀胱切除术的46例75岁以上患者,其中LRC组21例,ORC组25例。回顾性收集并分析两组患者的人口统计学参数、手术变量及围手术期结果。围手术期发病率和死亡率根据发生时间分为早期(术后90天内)或晚期(超过90天)。
两组患者术前特征具有可比性。与ORC组相比,LRC组手术时间明显更长(418 vs. 337分钟,p = 0.018),估计失血量更少(400 vs. 500毫升,p = 0.038)。感染和肠梗阻是术后最常见的早期并发症。术后90天内,接受ORC的患者发生肠梗阻(28.0% vs. 4.8%,P = 0.038)和感染(40% vs. 9.5%,P = 0.019)的比例明显高于LRC组。LRC组和ORC组的死亡率分别为4.7%(1/21)和4%(1/25)。中位随访21个月(范围2 - 61个月),Kaplan-Meier生存曲线和对数秩分析表明,LRC组和ORC组在3年总生存率、癌症特异性生存率或无复发生存率方面无显著差异。
对于预期寿命相对较长的老年患者,建议将LRC作为治疗肌层浸润性或高危非肌层浸润性膀胱癌的主要干预措施。