Figueroa Juan J, Singer Wolfgang, Parsaik Ajay, Benarroch Eduardo E, Ahlskog J Eric, Fealey Robert D, Parisi Joseph E, Sandroni Paola, Mandrekar Jay, Iodice Valeria, Low Phillip A, Bower James H
Department of Neurology, Medical College of Wisconsin, Milwaukee, WI.
Mov Disord. 2014 Aug;29(9):1151-7. doi: 10.1002/mds.25927. Epub 2014 Jun 7.
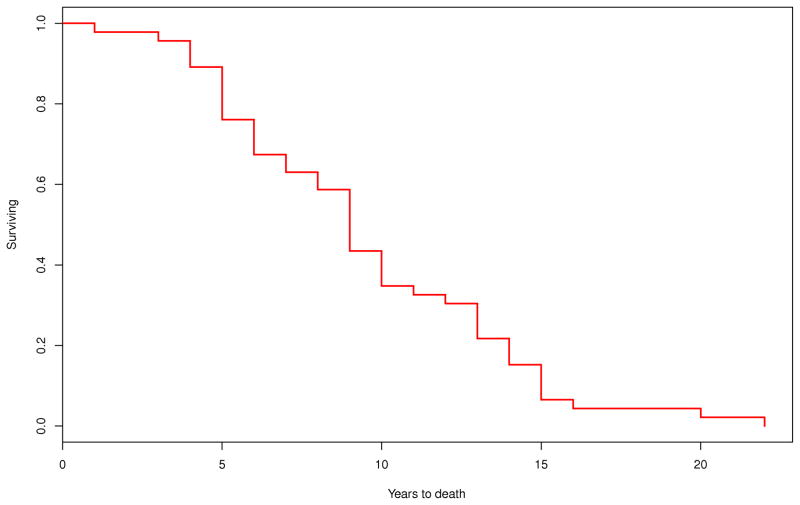
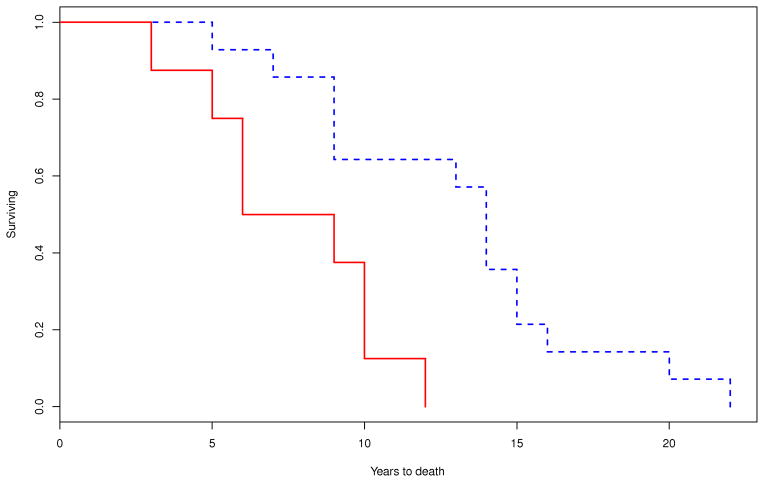
Neurological and autonomic presentation in multiple system atrophy (MSA) may predict early mortality. Quantification of early autonomic failure as a mortality predictor is lacking. Early neurological and autonomic clinical features were retrospectively reviewed in 49 MSA cases (median age at onset, 56.1 years; 16 women) confirmed by autopsy at Mayo Clinic. When available, the 10-point composite autonomic severity score derived from the autonomic reflex screen provided quantification of the degree of autonomic failure and thermoregulatory sweat test quantitated body surface anhidrosis. Symptoms at onset were autonomic in 50%, parkinsonian in 30%, and cerebellar in 20% of cases. Survival (median [95% confidence interval]) was 8.6 [6.7-10.2] years. Survival was shorter in patients with early laboratory evidence of generalized (composite autonomic severity score ≥ 6) autonomic failure (7.0 [3.9-9.8] vs. 9.8 [4.6-13.8] years; P = 0.036), and early requirement of bladder catheterization (7.3 [3.1-10.2] vs. 13.7 [8.5-14.9] years; P = 0.003) compared with those without these clinical features. On Cox proportional analysis, prognostic indicators of shorter survival were older age at onset (hazard ratio [95% confidence interval], 1.04 [1.01-1.08]; P = 0.03), early requirement of bladder catheterization (7.9 [1.88-38.63]; P = 0.004), and early generalized (composite autonomic severity score ≥ 6) autonomic failure (2.8 [1.01-9.26]; P = 0.047). Gender, phenotype, and early development of gait instability, aid-requiring ambulation, orthostatic symptoms, neurogenic bladder, or significant anhidrosis (thermoregulatory sweat test ≥ 40%) were not indicators of shorter survival. Our data suggest that early development of severe generalized autonomic failure more than triples the risk of shorter survival in patients with MSA.
多系统萎缩(MSA)中的神经和自主神经表现可能预示早期死亡。目前缺乏将早期自主神经功能衰竭量化作为死亡率预测指标的研究。对梅奥诊所经尸检确诊的49例MSA患者(发病年龄中位数为56.1岁;16例女性)的早期神经和自主神经临床特征进行了回顾性分析。如有可能,自主神经反射筛查得出的10分综合自主神经严重程度评分可量化自主神经功能衰竭的程度,而体温调节汗液试验可定量体表无汗情况。发病时症状为自主神经症状的病例占50%,帕金森症状的占30%,小脑症状的占20%。生存时间(中位数[95%置信区间])为8.6[6.7 - 10.2]年。与无这些临床特征的患者相比,早期有全身性(综合自主神经严重程度评分≥6)自主神经功能衰竭实验室证据的患者生存时间较短(7.0[3.9 - 9.8]年对9.8[4.6 - 13.8]年;P = 0.036),以及早期需要膀胱插管的患者生存时间较短(7.3[3.1 - 10.2]年对13.7[8.5 - 14.9]年;P = 0.003)。在Cox比例分析中,生存时间较短的预后指标为发病年龄较大(风险比[95%置信区间],1.04[1.01 - 1.08];P = 0.03)、早期需要膀胱插管(7.9[1.88 - 38.63];P = 0.004)以及早期全身性(综合自主神经严重程度评分≥6)自主神经功能衰竭(2.8[1.01 - 9.26];P = 0.047)。性别、表型以及步态不稳、需辅助行走、体位性症状、神经源性膀胱或显著无汗(体温调节汗液试验≥40%)的早期出现并非生存时间较短的指标。我们的数据表明,严重全身性自主神经功能衰竭的早期出现使MSA患者生存时间缩短的风险增加了两倍多。