Abdelhakim Kherfani, Khalil Amri, Haroune Bouhali, Oubaid Marzouk, Mondher Mestiri
Orthopedic Institute of MT Kassab, Tunisia.
Orthopedic Institute of MT Kassab, Tunisia.
Int J Surg Case Rep. 2014;5(7):434-6. doi: 10.1016/j.ijscr.2014.03.025. Epub 2014 May 2.
Hydatid cyst of bone constitutes only 0.5-2% of all hydatidoses. The thoracic spine is the most common site of spinal hydatidoses. Primary hydatid cyst of the sacral spinal canal is rare.
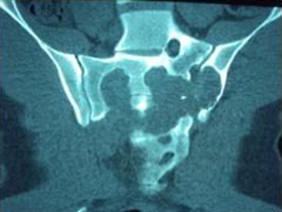
A 19-year-old man had cauda equina syndrome with pelvic pain 15 days ago, the pelvic radiography shows a lytic image depend on the left sacral wing. MRI showed an intra-pelvic cystic image invading the sacrum T1 hypointense and T2W hyperintense. The Hydatid serology was positive.Surgical treatment consisted of a wide drainage of hydatid cavity dug in the left sacral wing, and by which it communicated intra pelvic, with removal of the entire cyst by gentle aspiration, abundant rinsing with hypertonic saline, release and sacred roots encompassed in a puddle of fibrosis hydatid.The evolution was good with recovery of perineal sensation and anal tone. The sacroiliac joint was considered stable and did not require synthesis or reconstruction.
Hydatid cysts predominantly occur in liver and lungs. Involvement of other organs is uncommon. Neither surgery nor medical therapy is generally effective for bone, especially spinal hydatidosis. The initial treatment of choice is surgical excision for neural decompression and establishing diagnosis. Albendazole is the drug of choice against this disease, when suspected, presurgical use of Albendazole in Echinococcus infestations reduces risk of recurrence and/or facilitates surgery by reducing intracystic pressure.
A missed diagnosis of hydatid cyst could be devastating. Hence, hydatid cyst should be kept as a differential diagnosis, when encountered with a cystic lesion of sacrum. In addition, longterm follow-up is mandatory as recurrence is high despite use scolicidal agents.
骨包虫囊肿仅占所有包虫病的0.5%-2%。胸椎是脊柱包虫病最常见的部位。骶管原发性包虫囊肿罕见。
一名19岁男性15天前出现马尾综合征伴盆腔疼痛,盆腔X线片显示左侧骶骨翼有溶骨性影像。MRI显示盆腔内囊性影像侵犯骶骨,T1加权像呈低信号,T2加权像呈高信号。包虫血清学检查呈阳性。手术治疗包括在左侧骶骨翼广泛引流包虫腔,该腔与盆腔相通,通过轻柔抽吸清除整个囊肿,用高渗盐水充分冲洗,松解并将骶神经根包裹在包虫纤维化灶中。恢复良好,会阴感觉和肛门张力恢复。骶髂关节被认为稳定,无需进行固定或重建。
包虫囊肿主要发生在肝脏和肺部。累及其他器官并不常见。对于骨包虫病,尤其是脊柱包虫病,手术和药物治疗通常都无效。最初的治疗选择是手术切除以解除神经压迫并明确诊断。阿苯达唑是治疗该病的首选药物,当怀疑感染时,术前使用阿苯达唑可降低复发风险和/或通过降低囊内压力便于手术。
包虫囊肿漏诊可能是灾难性的。因此,当遇到骶骨囊性病变时,应将包虫囊肿作为鉴别诊断之一。此外,尽管使用了杀头节剂,但复发率较高,因此必须进行长期随访。