1] Division of Urology, Department of Surgical Oncology, Princess Margaret Cancer Centre, 610 University Avenue, Toronto, Ontario, Canada M5G 2M9 [2] Division of Urology, Department of Surgery, University Health Network, University of Toronto, 610 University Avenue, Toronto, Ontario, Canada M5G 2M9.
1] Division of Urology, Department of Surgery, University Health Network, University of Toronto, 610 University Avenue, Toronto, Ontario, Canada M5G 2M9 [2] Institute for Clinical Evaluative Sciences, 2075 Bayview Avenue, Toronto, Ontario, Canada M4N 3M5.
Br J Cancer. 2014 Jul 29;111(3):444-51. doi: 10.1038/bjc.2014.305. Epub 2014 Jun 10.
An elevated neutrophil-to-lymphocyte ratio (NLR) is associated with poor outcome in various tumours. Its prognostic utility in patients with urothelial carcinoma of the bladder (UCB) undergoing radical cystectomy (RC) is yet to be fully elucidated.
A cohort of patients undergoing RC for UCB in a tertiary referral centre between 1992 and 2012 was analysed. Neutrophil-to-lymphocyte ratio was computed using complete blood counts performed pre-RC, or before neo-adjuvant chemotherapy where applicable. Time-dependent receiver operating characteristic curves were used to determine the optimal cutoff point for predicting recurrence-free survival (RFS), cancer-specific survival (CSS) and overall survival (OS). The predictive ability of NLR was assessed using Kaplan-Meier analyses and multivariable Cox proportional hazards models. The likelihood-ratio test was used to determine whether multivariable models were improved by including NLR.
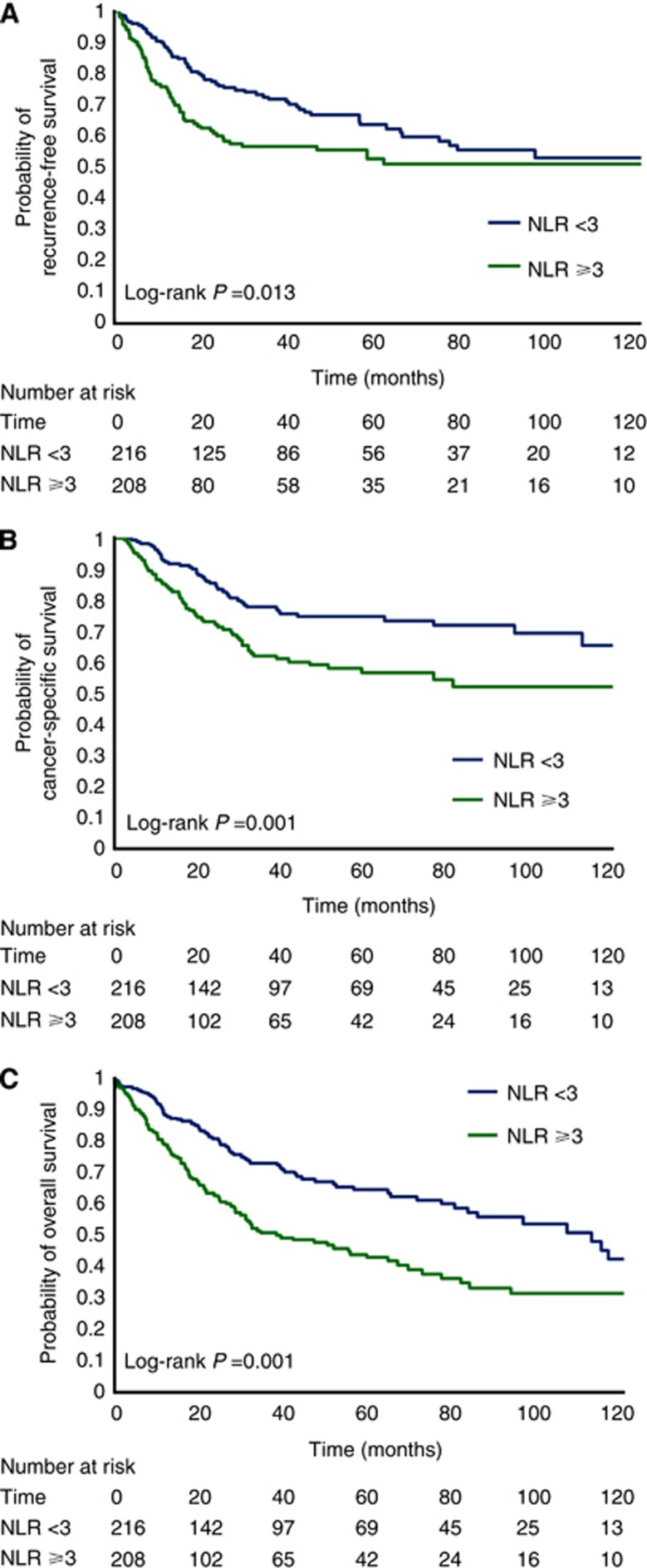
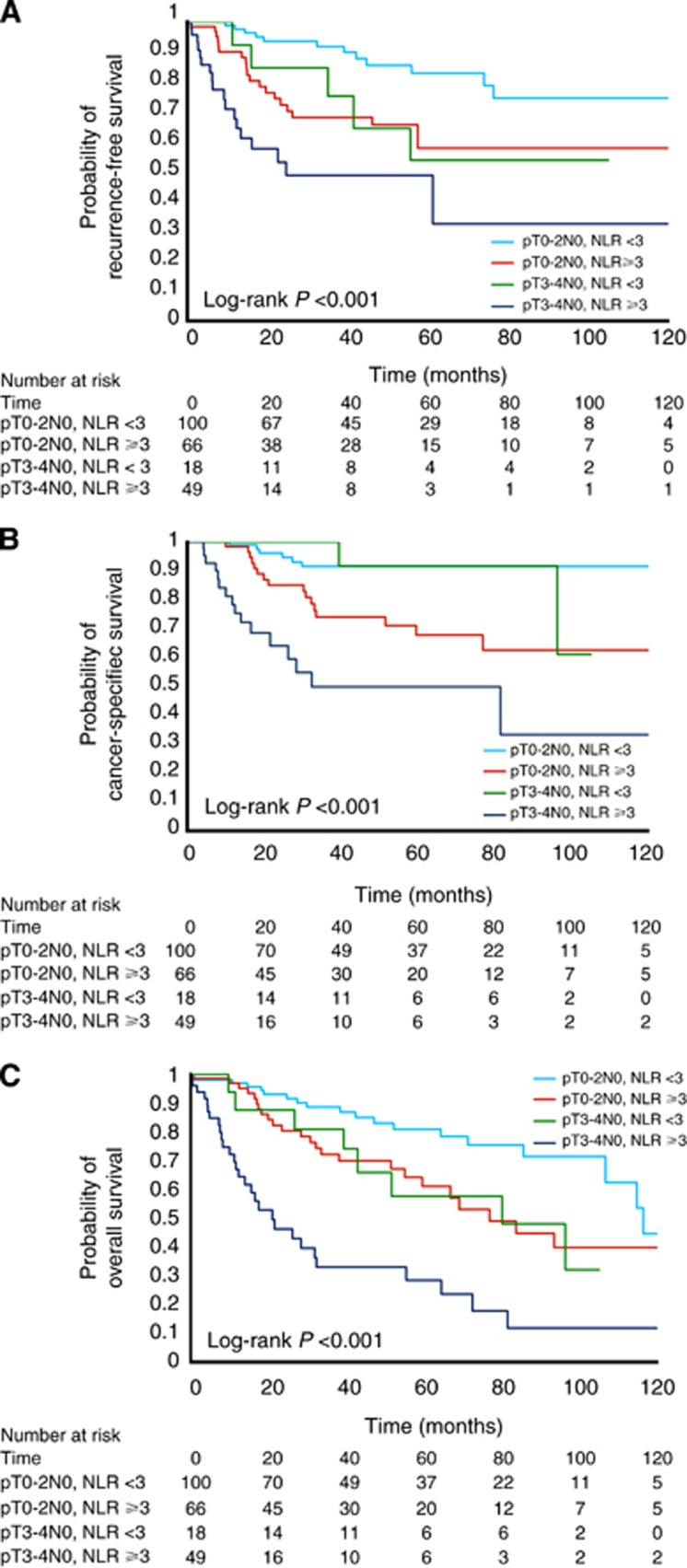
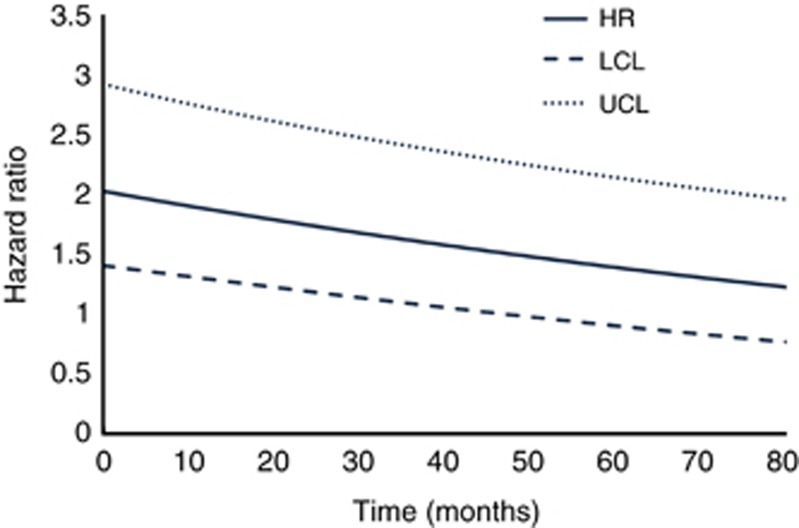
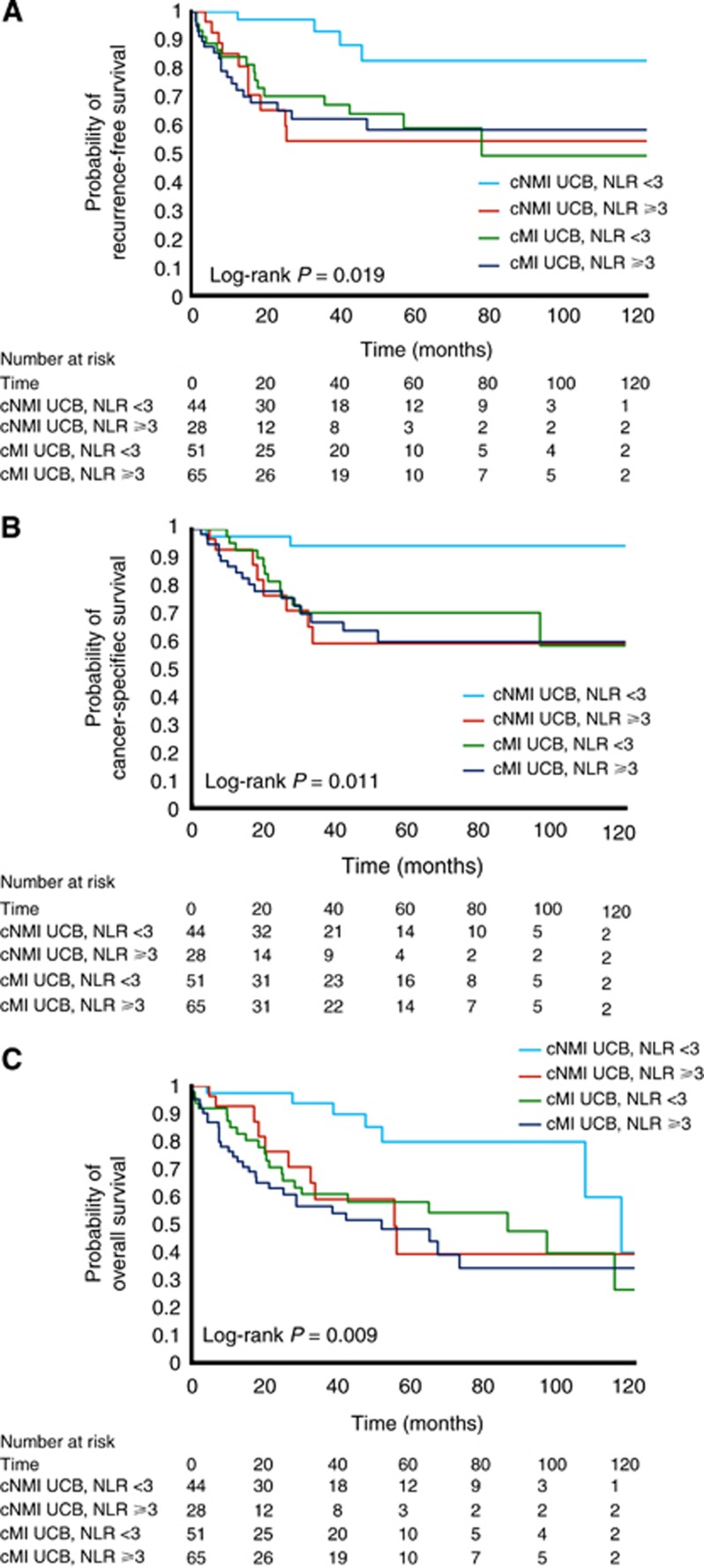
The cohort included 424 patients followed for a median of 58.4 months. An NLR of 3 was determined as the optimal cutoff value. Patients with an NLR⩾3.0 had significantly worse survival outcomes (5y-RFS: 53% vs 64%, log-rank P=0.013; 5y-CSS: 57% vs 75%, log-rank P<0.001; 5y-OS: 43% vs 64%, log-rank P<0.001). After adjusting for disease-specific predictors, an NLR ⩾3.0 was significantly associated with worse RFS (HR=1.49; 95% CI=1.12-2.0, P=0.007), CSS (HR=1.88; 95% CI=1.39-2.54, P<0.001) and OS (average HR=1.67; 95% CI=1.17-2.39, P=0.005). The likelihood-ratio test confirmed that prognostic models were improved by including NLR.
Neutrophil-to-lymphocyte ratio is an inexpensive prognostic biomarker for patients undergoing RC for UCB. It offers pre-treatment prognostic value in addition to established prognosticators and may be helpful in guiding treatment decisions.
中性粒细胞与淋巴细胞比值(NLR)升高与多种肿瘤的不良预后相关。其在接受根治性膀胱切除术(RC)的膀胱癌患者中的预后作用尚未完全阐明。
分析了 1992 年至 2012 年期间在三级转诊中心接受 RC 治疗的膀胱癌患者队列。RC 前或新辅助化疗前(如有)的全血细胞计数计算 NLR。使用时间依赖性接收者操作特征曲线确定预测无复发生存(RFS)、癌症特异性生存(CSS)和总生存(OS)的最佳截断值。使用 Kaplan-Meier 分析和多变量 Cox 比例风险模型评估 NLR 的预测能力。似然比检验用于确定是否通过包含 NLR 来改善多变量模型。
该队列包括 424 例患者,中位随访时间为 58.4 个月。确定 NLR 为 3 是最佳截断值。NLR ⩾3.0 的患者生存结局明显较差(5y-RFS:53% vs 64%,对数秩检验 P=0.013;5y-CSS:57% vs 75%,对数秩检验 P<0.001;5y-OS:43% vs 64%,对数秩检验 P<0.001)。在校正疾病特异性预测因素后,NLR ⩾3.0 与 RFS(HR=1.49;95%CI=1.12-2.0,P=0.007)、CSS(HR=1.88;95%CI=1.39-2.54,P<0.001)和 OS(平均 HR=1.67;95%CI=1.17-2.39,P=0.005)显著相关。似然比检验证实,通过包含 NLR,预后模型得到改善。
中性粒细胞与淋巴细胞比值是接受 RC 治疗膀胱癌患者的一种廉价的预后生物标志物。它在提供既定预后指标之外,还具有治疗前预后价值,可能有助于指导治疗决策。