Lund Caterina A, Møller Ann M, Wetterslev Jørn, Lundstrøm Lars H
Department of Anaesthesia and Intensive Care, Herlev University Hospital, Herlev, Denmark.
Copenhagen Trial Unit, Centre for Clinical Intervention Research, Rigshospitalet, Copenhagen University Hospital, København, Denmark.
PLoS One. 2014 Jun 13;9(6):e99308. doi: 10.1371/journal.pone.0099308. eCollection 2014.
In hospital and health care organizational factors may be changed to reduce postoperative mortality. The aim of this study is to evaluate a possible association between mortality and 'length of hospital stay', 'priority of surgery', 'time of surgery', or 'surgical delay' in hip fracture surgery.
Observational cohort study.
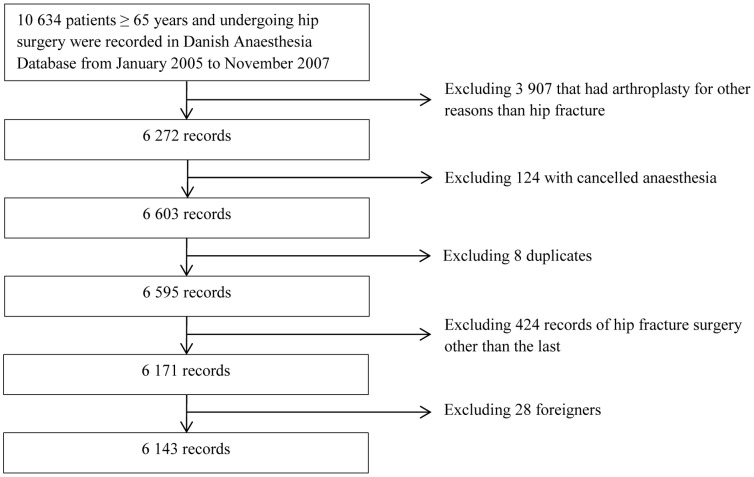
Prospectively and consecutively reported data from the Danish Anaesthesia Database were linked to The Danish National Registry of Patients and The Civil Registration System. Records on vital status, admittance, discharges, codes of diagnosis, anaesthetic and surgical procedures were retrieved.
6143 patients aged more than 65 years undergoing hip fracture surgery.
All-cause mortality.
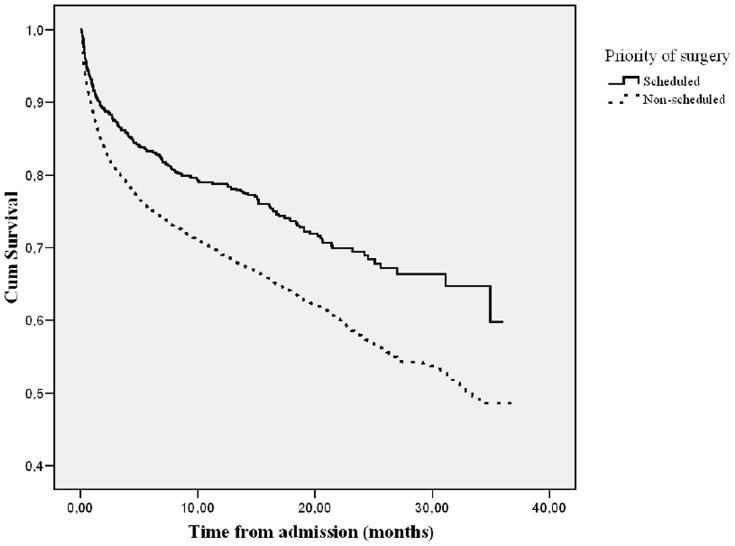
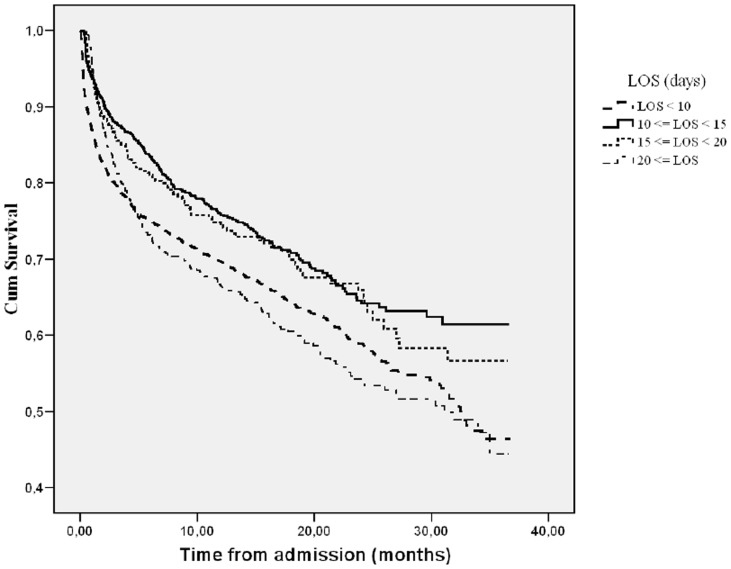
The one year mortality was 30% (28-31%, 95% Confidence interval (CI)). In a multivariate model 'length of hospital stay' less than 10 days and more than 20 days are associated with mortality with hazard ratios of 1.34 (1.20-1.53 CI, p<0.001) and 1.27 (1.06-1.51 CI, p<0.001), respectively. 'Priority of surgery' categorized as 'non-scheduled' is associated with mortality with a hazard ratio of 1.31 (1.13-1.50 CI, p<0.001). Surgical delay and time of surgery are not significantly associated with mortality.
Non-scheduled surgery and length of hospital stay were associated with increased mortality. Confounding by indication may bias observational studies evaluating early and late discharge as well as priority; therefore cluster randomized clinical trials comparing different clinical set ups may be warranted evaluating health care organizational factors.
医院及医疗保健机构的组织因素可加以改变以降低术后死亡率。本研究旨在评估髋部骨折手术中死亡率与“住院时间”“手术优先级”“手术时间”或“手术延迟”之间可能存在的关联。
观察性队列研究。
丹麦麻醉数据库前瞻性且连续报告的数据与丹麦国家患者登记处及民事登记系统相链接。检索了有关生命状态、入院、出院、诊断编码、麻醉及外科手术的记录。
6143名年龄超过65岁接受髋部骨折手术的患者。
全因死亡率。
一年死亡率为30%(28 - 31%,95%置信区间(CI))。在多变量模型中,住院时间少于10天和超过20天与死亡率相关,风险比分别为1.34(1.20 - 1.53 CI,p < 0.001)和1.27(1.06 - 1.51 CI,p < 0.001)。分类为“非计划”的“手术优先级”与死亡率相关,风险比为1.31(1.13 - 1.50 CI,p < 0.001)。手术延迟和手术时间与死亡率无显著关联。
非计划手术和住院时间与死亡率增加相关。指征性混杂因素可能会使评估早期和晚期出院以及优先级的观察性研究产生偏差;因此,可能需要进行比较不同临床设置的整群随机临床试验来评估医疗保健机构的组织因素。